

Immune-Related Adverse Effects of Cancer Immunotherapy- Implications for Rheumatology
- PMID: 27890174
- PMCID: PMC5127444
- DOI: 10.1016/j.rdc.2016.09.007
Immune-Related Adverse Effects of Cancer Immunotherapy- Implications for Rheumatology
Abstract
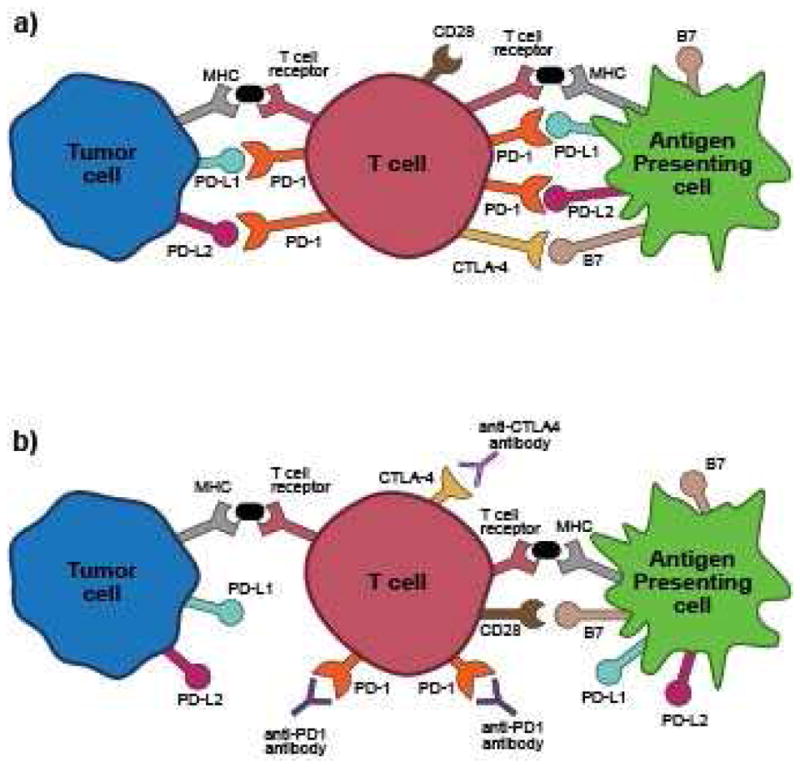
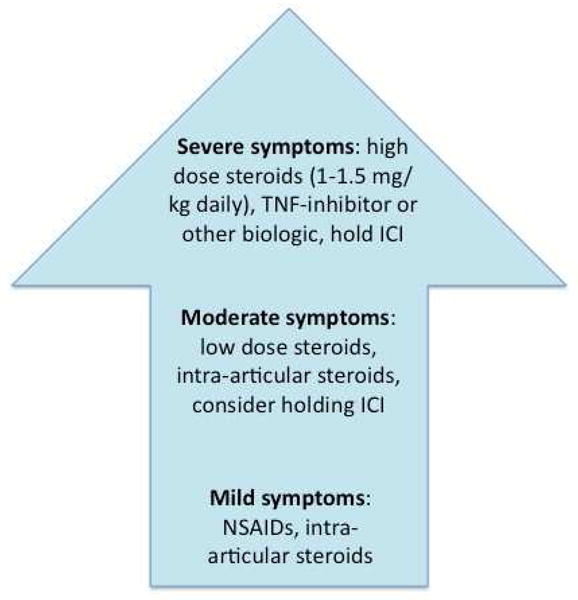
Immune checkpoint inhibitors (ICIs) are increasingly studied and used as therapy for a growing number of malignancies. ICIs work by blocking inhibitory pathways of T-cell activation, leading to an immune response directed against tumors. Such nonspecific immunologic activation can lead to immune-related adverse events (IRAEs). Some IRAEs, including inflammatory arthritis, sicca syndrome, myositis, and vasculitis, are of special interest to rheumatologists. As use of ICIs increases, recognition of these IRAEs and developing treatment strategies will become important. In this review, the current literature on rheumatic and musculoskeletal IRAEs is summarized. The incidence, clinical presentations, and treatment considerations are highlighted.
Keywords: Arthritis; Immune checkpoint inhibitors; Immune-related adverse events; Malignancy; Sicca syndrome.
Copyright © 2016 Elsevier Inc. All rights reserved.
Conflict of interest statement
Dr. Bingham has served as a consultant for Bristol-Myers-Squibb.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
