

The anatomical perspective of human occipital condyle in relation to the hypoglossal canal, condylar canal, and jugular foramen and its surgical significance
- PMID: 27891034
- PMCID: PMC5111326
- DOI: 10.4103/0974-8237.193258
The anatomical perspective of human occipital condyle in relation to the hypoglossal canal, condylar canal, and jugular foramen and its surgical significance
Abstract
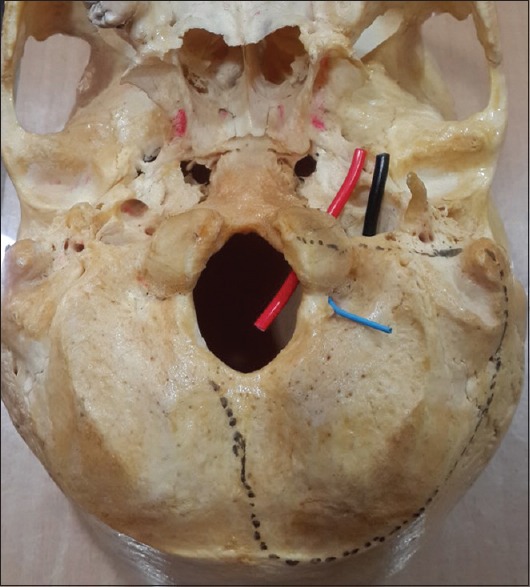
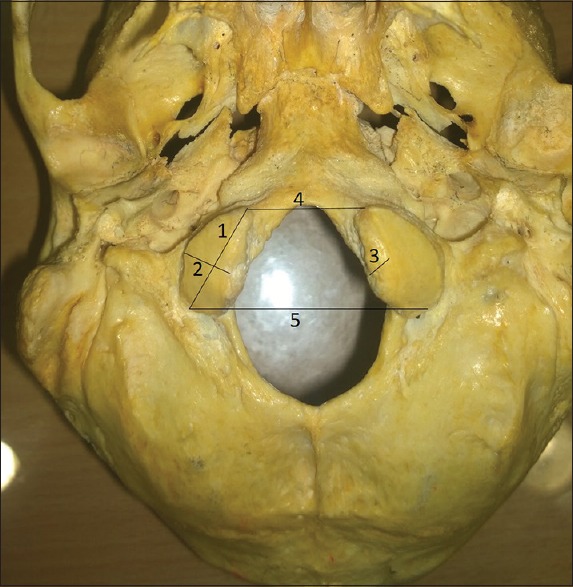
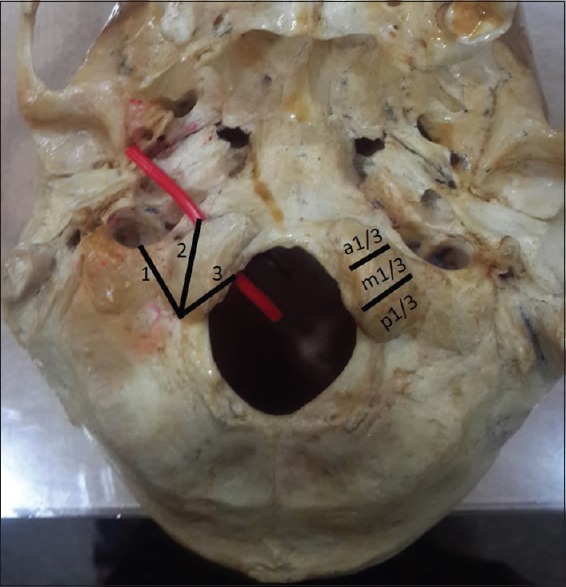
Background: The transcondylar approach (TCA) has gained importance in recent era which enables shorter and direct route to access the lesions ventral to the brainstem. The important step in this approach is resection of the occipital condyle (OC). The detailed knowledge of bony anatomy of OC and its relation to the hypoglossal canal (HC), condylar canal (CC), and jugular foramen (JF) is very important to avoid any iatrogenic injury during craniovertebral surgeries. The aim of the present study is to conduct a morphometric and morphological study and note the variations of the OC and the structures surrounding it in North Indian population.
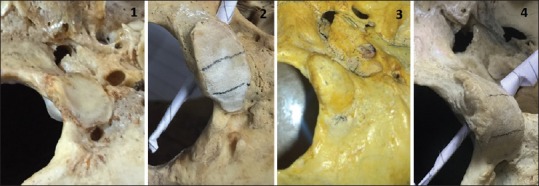
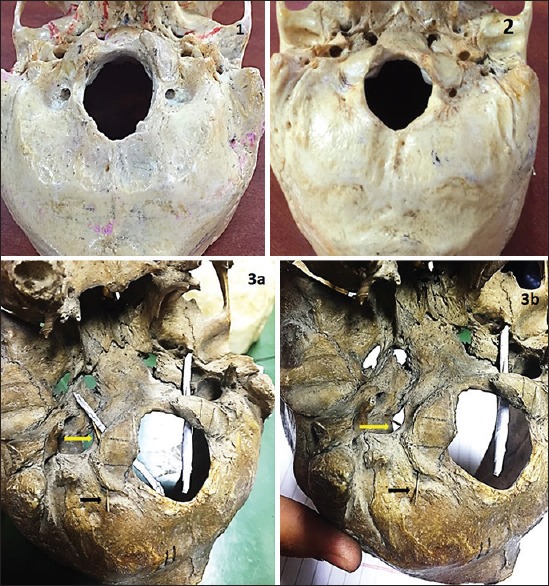
Materials and methods: The study was carried out on 100 OC. Morphometric measurements of OC and the distances of HC and JF from the posterior end of OC were noted. In addition, the extent of the HC and JF in relation to OC, presence or absence of CC, shape of the OC, and its articular facet were also noted.
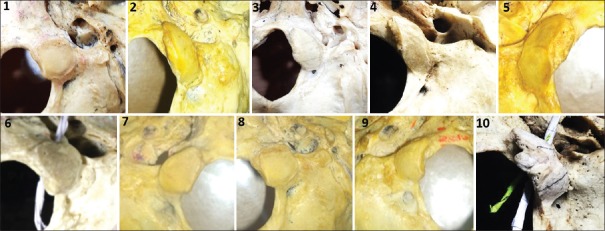
Results: The incidence of short OC was seen in 13% skulls. The most common shape of OC was oval or rhomboid. Even though the articular facet was convex in majority of skulls but flat (10%) and concave (1%) were also observed. The external and internal distance of HC from the posterior end of OC was13.83 mm and 10.66 mm on the right side and 15.02 mm and 11.89 mm on the left side. The OC was related in its middle 1/3 to the HC in 15% skulls and to the whole extent of JF in 3% skulls. Thirty-four percent skulls displayed the septa in the HC. The CC was present bilaterally in 38% skulls and unilaterally in 40% skulls.
Conclusion: The OC and related structures such as HC, CC, and JF are likely to have variations in respect to morphometry and morphology. This study may prove helpful to neurosurgeons operating in this field, especially during TCA where neurovascular structures emerging from these canals and foramen are more vulnerable to injury.
Keywords: Condylar canal; hypoglossal canal; jugular foramen; occipital condyle; transcondylar approach.
Figures
Similar articles
-
Morphological analysis and morphometry of the occipital condyle and its relationship to the foramen magnum, jugular foramen, and hypoglossal canal: implications for craniovertebral junction surgery.Anat Cell Biol. 2023 Mar 31;56(1):61-68. doi: 10.5115/acb.22.105. Epub 2023 Jan 13. Anat Cell Biol. 2023. PMID: 36635090 Free PMC article.
-
A morphometric analysis of the foramen magnum region as it relates to the transcondylar approach.Acta Neurochir (Wien). 2005 Aug;147(8):889-95. doi: 10.1007/s00701-005-0555-x. Epub 2005 Jun 9. Acta Neurochir (Wien). 2005. PMID: 15924208
-
Anatomic study of the occipital condyle and its surgical implications in transcondylar approach.J Craniovertebr Junction Spine. 2014 Apr;5(2):71-7. doi: 10.4103/0974-8237.139201. J Craniovertebr Junction Spine. 2014. PMID: 25210336 Free PMC article.
-
Common surgical pitfalls in the skull.Surg Neurol. 2003 Mar;59(3):228-31; discussion 231. doi: 10.1016/s0090-3019(02)01038-8. Surg Neurol. 2003. PMID: 12681561 Review.
-
Catalogue of the Skulls of Various Nations.Br Foreign Med Chir Rev. 1860 Jul;26(51):87-92. Br Foreign Med Chir Rev. 1860. PMID: 30163392 Free PMC article. Review. No abstract available.
Cited by
-
Dural arteriovenous fistula of the lateral foramen magnum region: A review.Interv Neuroradiol. 2018 Aug;24(4):425-434. doi: 10.1177/1591019918770768. Epub 2018 May 4. Interv Neuroradiol. 2018. PMID: 29726736 Free PMC article. Review.
-
Immersive Surgical Anatomy of the Far-Lateral Approach.Cureus. 2022 Nov 8;14(11):e31257. doi: 10.7759/cureus.31257. eCollection 2022 Nov. Cureus. 2022. PMID: 36514632 Free PMC article.
-
Morphometric analysis of posterior cranial fossa and surgical implications.J Craniovertebr Junction Spine. 2021 Apr-Jun;12(2):178-182. doi: 10.4103/jcvjs.jcvjs_205_20. Epub 2021 Jun 10. J Craniovertebr Junction Spine. 2021. PMID: 34194165 Free PMC article.
-
The condylar canal and emissary vein-a comprehensive and pictorial review of its anatomy and variation.Childs Nerv Syst. 2019 May;35(5):747-751. doi: 10.1007/s00381-019-04120-4. Epub 2019 Mar 21. Childs Nerv Syst. 2019. PMID: 30900022 Review.
-
Morphological analysis and morphometry of the occipital condyle and its relationship to the foramen magnum, jugular foramen, and hypoglossal canal: implications for craniovertebral junction surgery.Anat Cell Biol. 2023 Mar 31;56(1):61-68. doi: 10.5115/acb.22.105. Epub 2023 Jan 13. Anat Cell Biol. 2023. PMID: 36635090 Free PMC article.
References
-
- Standring S. Head and neck: Overview and surface anatomy. In: Gleeson M, Tunstall R, editors. Gray's Anatomy. The Anatomical Basis of Clinical Practice. 40th ed. Edinburg: Churchill and Livingston; 2008. pp. 415–6.
-
- Vishteh AG, Crawford NR, Melton MS, Spetzler RF, Sonntag VK, Dickman CA. Stability of the craniovertebral junction after unilateral occipital condyle resection: A biomechanical study. J Neurosurg. 1999;90(1 Suppl):91–8. - PubMed
-
- Boulton MR, Cusimano MD. Foramen magnum meningiomas: Concepts, classifications, and nuances. Neurosurg Focus. 2003;14:e10. - PubMed
-
- Wen HT, Rhoton AL, Jr, Katsuta T, de Oliveira E. Microsurgical anatomy of the transcondylar, supracondylar, and paracondylar extensions of the far-lateral approach. J Neurosurg. 1997;87:555–85. - PubMed
-
- Avci E, Dagtekin A, Ozturk AH, Kara E, Ozturk NC, Uluc K, et al. Anatomical variations of the foramen magnum, occipital condyle and jugular tubercle. Turk Neurosurg. 2011;21:181–90. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
