

Optimising Antibiotic Usage to Treat Bacterial Infections
- PMID: 27892497
- PMCID: PMC5124968
- DOI: 10.1038/srep37853
Optimising Antibiotic Usage to Treat Bacterial Infections
Abstract
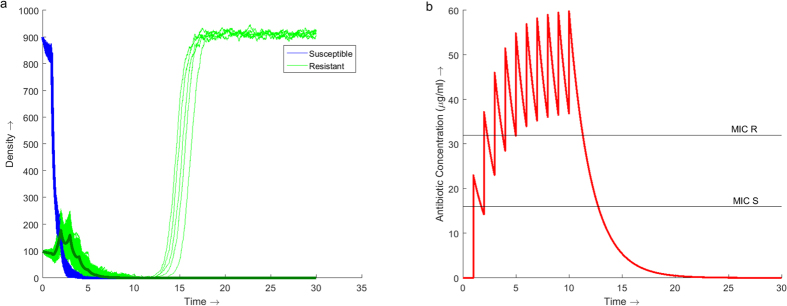
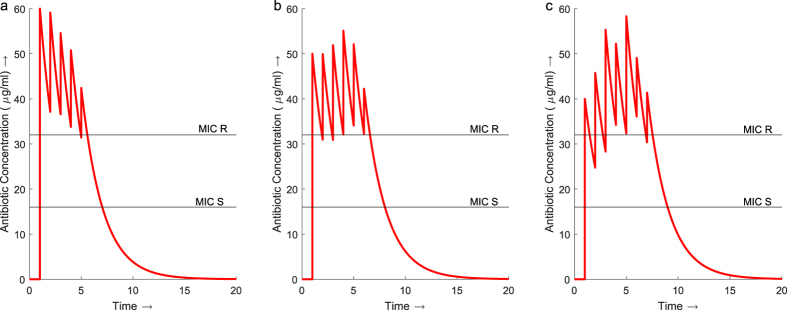
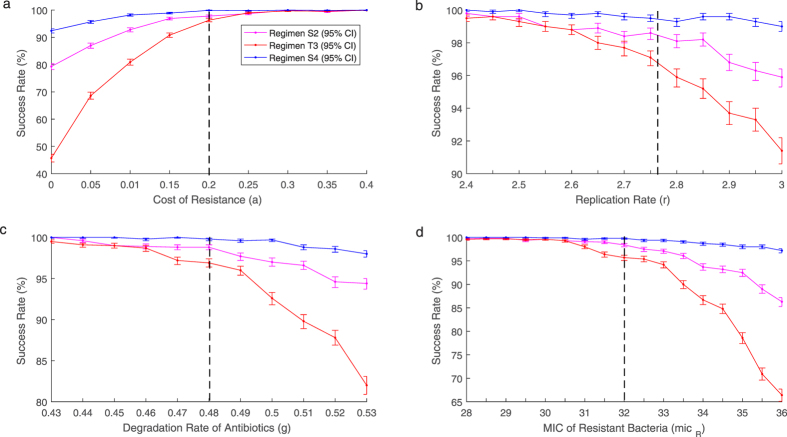
The increase in antibiotic resistant bacteria poses a threat to the continued use of antibiotics to treat bacterial infections. The overuse and misuse of antibiotics has been identified as a significant driver in the emergence of resistance. Finding optimal treatment regimens is therefore critical in ensuring the prolonged effectiveness of these antibiotics. This study uses mathematical modelling to analyse the effect traditional treatment regimens have on the dynamics of a bacterial infection. Using a novel approach, a genetic algorithm, the study then identifies improved treatment regimens. Using a single antibiotic the genetic algorithm identifies regimens which minimise the amount of antibiotic used while maximising bacterial eradication. Although exact treatments are highly dependent on parameter values and initial bacterial load, a significant common trend is identified throughout the results. A treatment regimen consisting of a high initial dose followed by an extended tapering of doses is found to optimise the use of antibiotics. This consistently improves the success of eradicating infections, uses less antibiotic than traditional regimens and reduces the time to eradication. The use of genetic algorithms to optimise treatment regimens enables an extensive search of possible regimens, with previous regimens directing the search into regions of better performance.
Figures
References
-
- Teillant A., Gandra S., Barter D., Morgan D. J. & Laxminarayan R. Potential burden of antibiotic resistance on surgery and cancer chemotherapy antibiotic prophylaxis in the USA: A literature review and modelling study. Lancet Infect. Dis. 15, 1429–1437 (2015). - PubMed
-
- Boucher H. W. et al. Bad bugs, no drugs: no ESKAPE! An update from the Infectious Diseases Society of America. Clin. Infect. Dis. 48, 1–12 (2009). - PubMed
-
- Ferber D. Superbugs on the Hoof? Science 288, 792–794 (2000). - PubMed
-
- Aarestrup F. M. Veterinary drug usage and antimicrobial resistance in bacteria of animal origin. Basic Clin. Pharmacol. Toxicol. 96, 271–281 (2005). - PubMed
-
- Cabello F. C. Heavy use of prophylactic antibiotics in aquaculture: a growing problem for human and animal health and for the environment. Environ. Microbiol. 8, 1137–44 (2006). - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
