

Functional and Structural Signatures of the Anterior Insula are associated with Risk-taking Tendency of Analgesic Decision-making
- PMID: 27892543
- PMCID: PMC5124953
- DOI: 10.1038/srep37816
Functional and Structural Signatures of the Anterior Insula are associated with Risk-taking Tendency of Analgesic Decision-making
Abstract
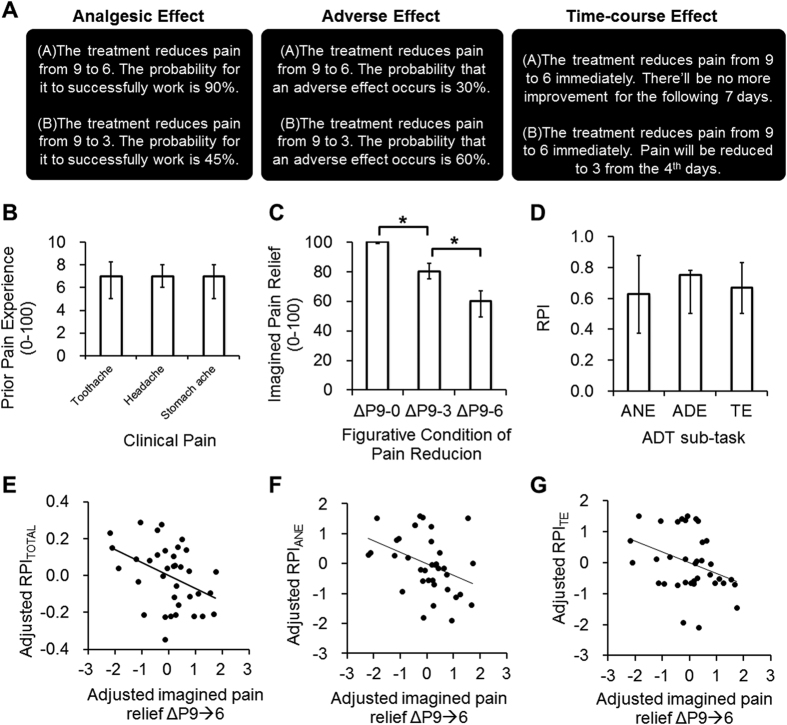
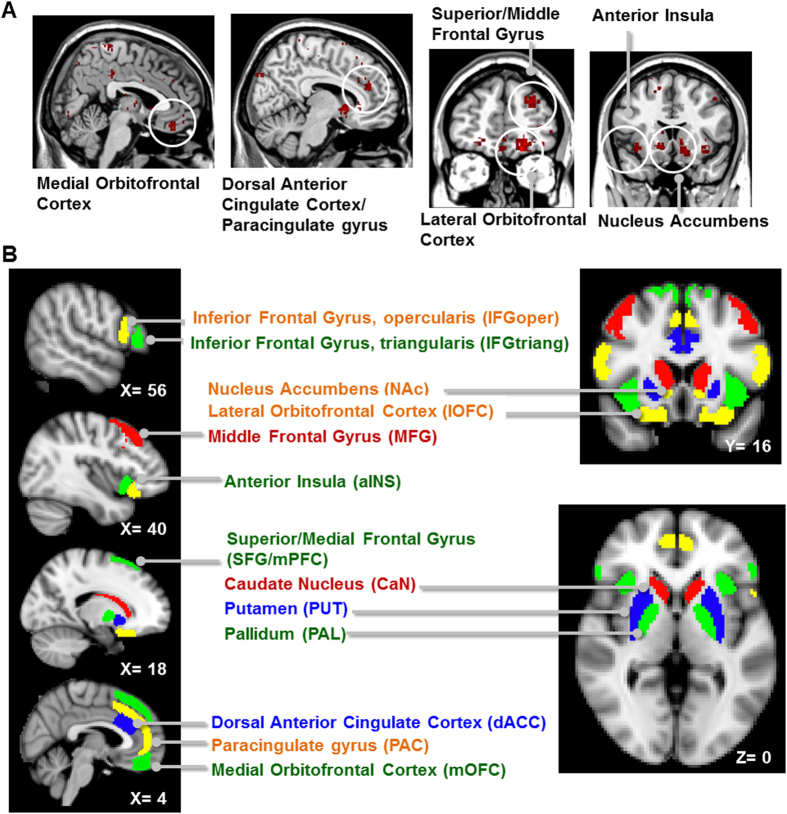
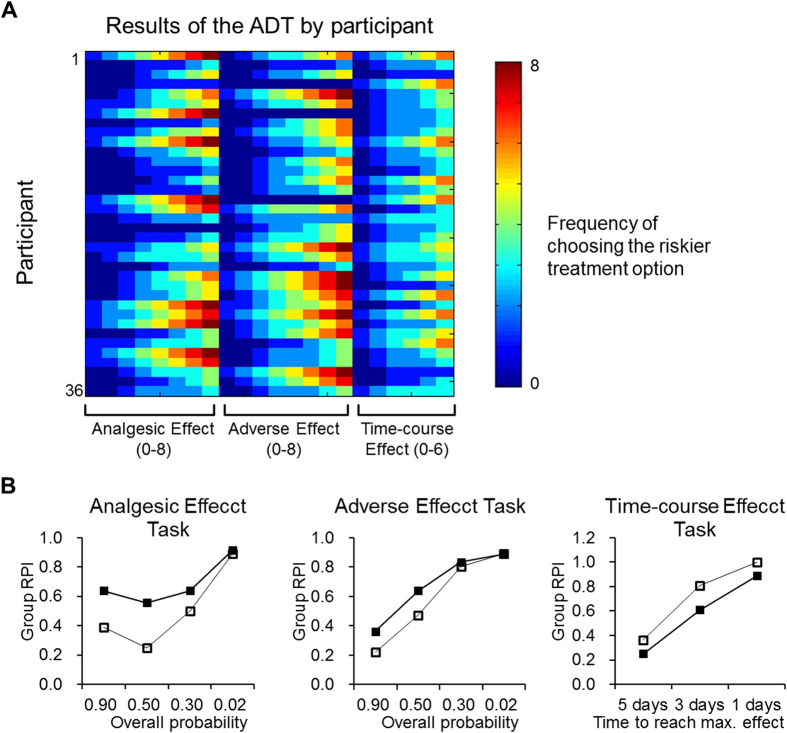
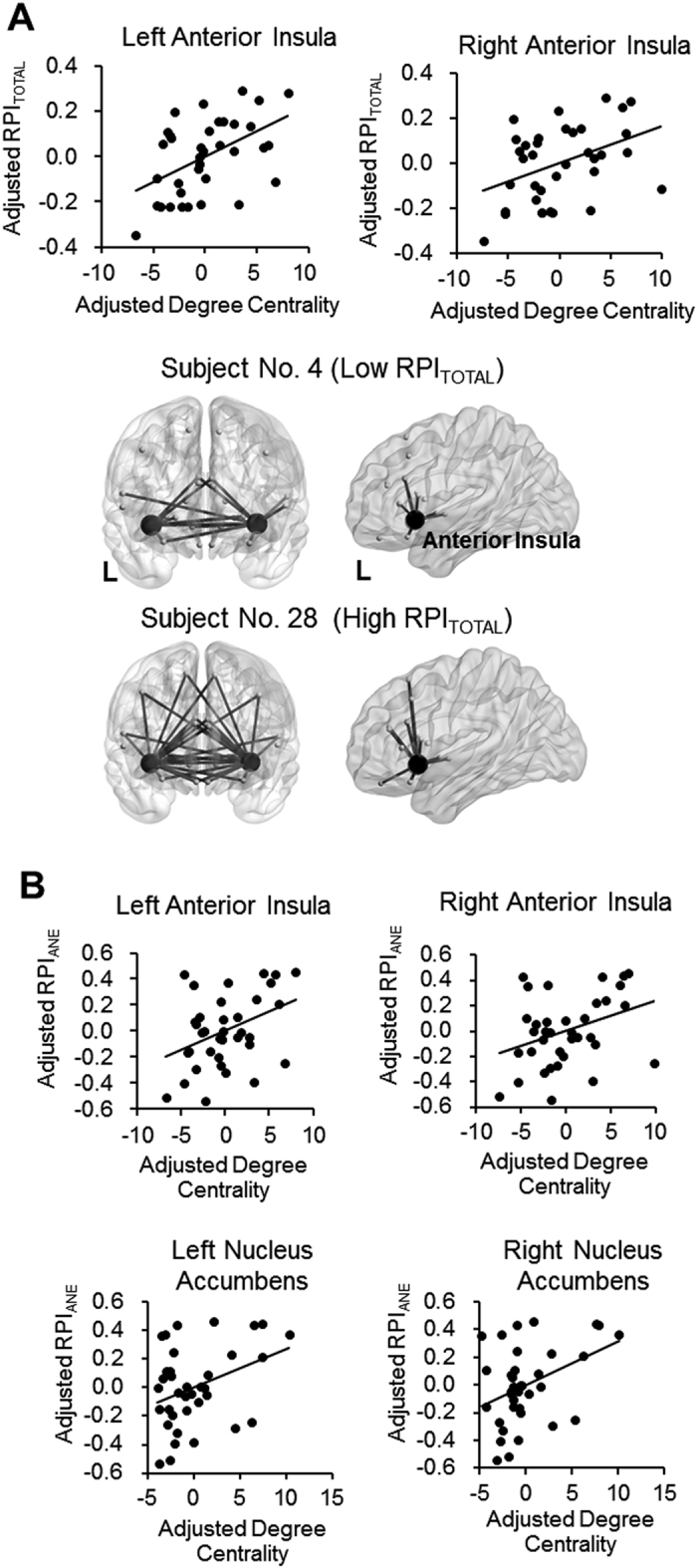
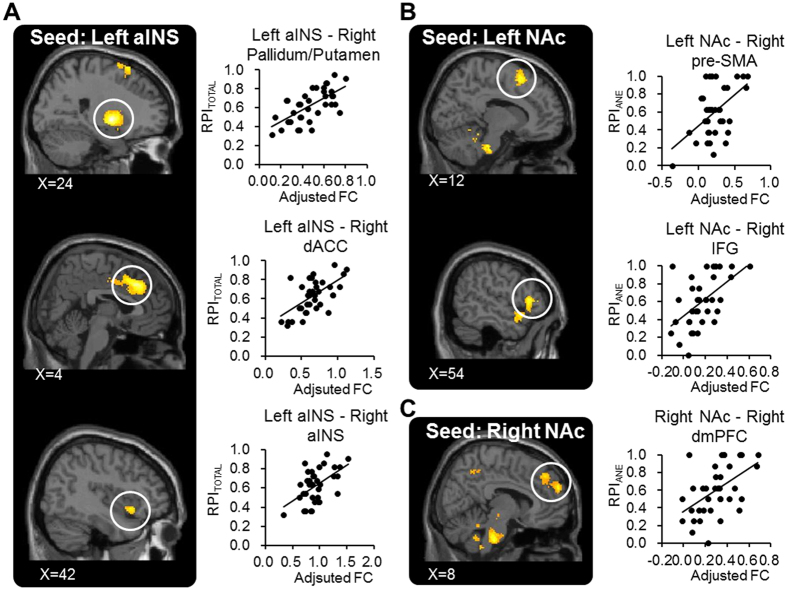
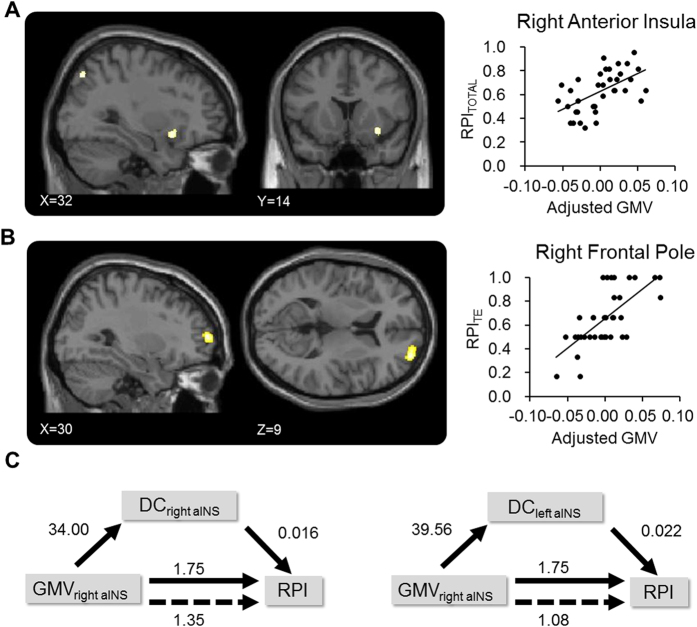
In a medical context, decision-making is associated with complicated assessment of gains, losses and uncertainty of outcomes. We here provide novel evidence about the brain mechanisms underlying decision-making of analgesic treatment. Thirty-six healthy participants were recruited and completed the Analgesic Decision-making Task (ADT), which quantified individual tendency of risk-taking (RPI), as the frequency of choosing a riskier option to relieve pain. All the participants received resting-state (rs) functional magnetic resonance imaging (MRI) and structural MRI. On rs-functional connectome, degree centrality (DC) of the bilateral anterior insula (aINS) was positively correlated with the RPI. The functional connectivity between the aINS, the nucleus accumbens and multiple brain regions, predominantly the medial frontal cortex, was positively correlated with the RPI. On structural signatures, the RPI was positively correlated with grey matter volume at the right aINS, and such an association was mediated by DC of the left aINS. Regression analyses revealed that both DC of the left aINS and participants' imagined pain relief, as the utility of pain reduction, could predict the individual RPI. The findings suggest that the functional and structural brain signature of the aINS is associated with the individual differences of risk-taking tendency in the context of analgesic decision-making.
Figures
References
-
- Frosch D. L. & Kaplan R. M. Shared decision making in clinical medicine: past research and future directions. American journal of preventive medicine 17, 285–294 (1999). - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
