

Development and Initial Validation of the Risk Analysis Index for Measuring Frailty in Surgical Populations
- PMID: 27893030
- PMCID: PMC7140150
- DOI: 10.1001/jamasurg.2016.4202
Development and Initial Validation of the Risk Analysis Index for Measuring Frailty in Surgical Populations
Abstract
Importance: Growing consensus suggests that frailty-associated risks should inform shared surgical decision making. However, it is not clear how best to screen for frailty in preoperative surgical populations.
Objective: To develop and validate the Risk Analysis Index (RAI), a 14-item instrument used to measure surgical frailty. It can be calculated prospectively (RAI-C), using a clinical questionnaire, or retrospectively (RAI-A), using variables from the surgical quality improvement databases (Veterans Affairs or American College of Surgeons National Surgical Quality Improvement Projects).
Design, setting, and participants: Single-site, prospective cohort from July 2011 to September 2015 at the Veterans Affairs Nebraska-Western Iowa Heath Care System, a Level 1b Veterans Affairs Medical Center. The study included all patients presenting to the medical center for elective surgery.
Exposures: We assessed the RAI-C for all patients scheduled for surgery, linking these scores to administrative and quality improvement data to calculate the RAI-A and the modified Frailty Index.
Main outcomes and measures: Receiver operator characteristics and C statistics for each measure predicting postoperative mortality and morbidity.
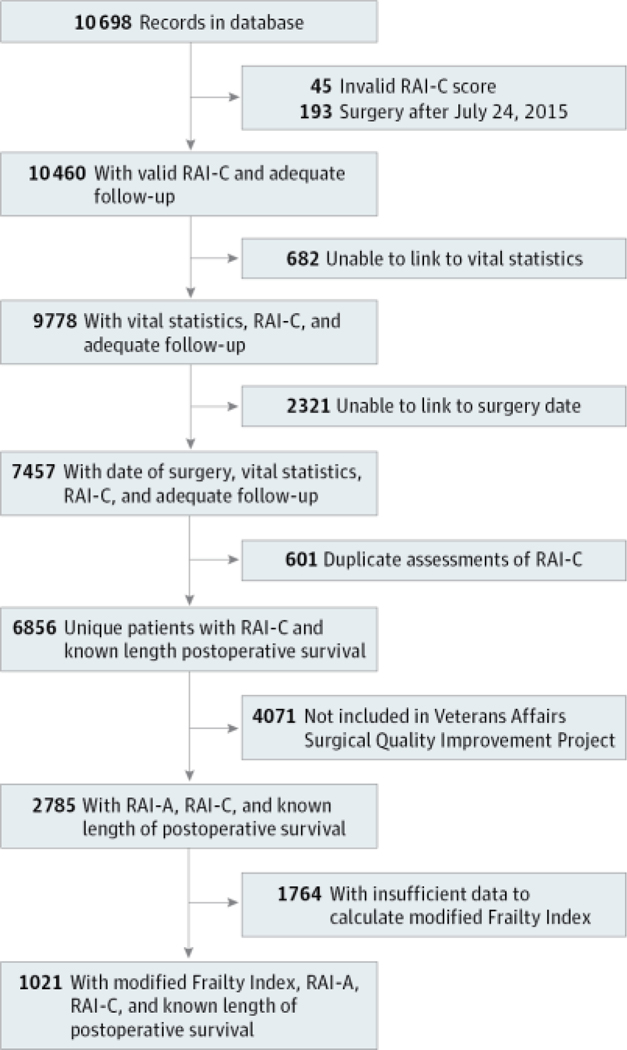
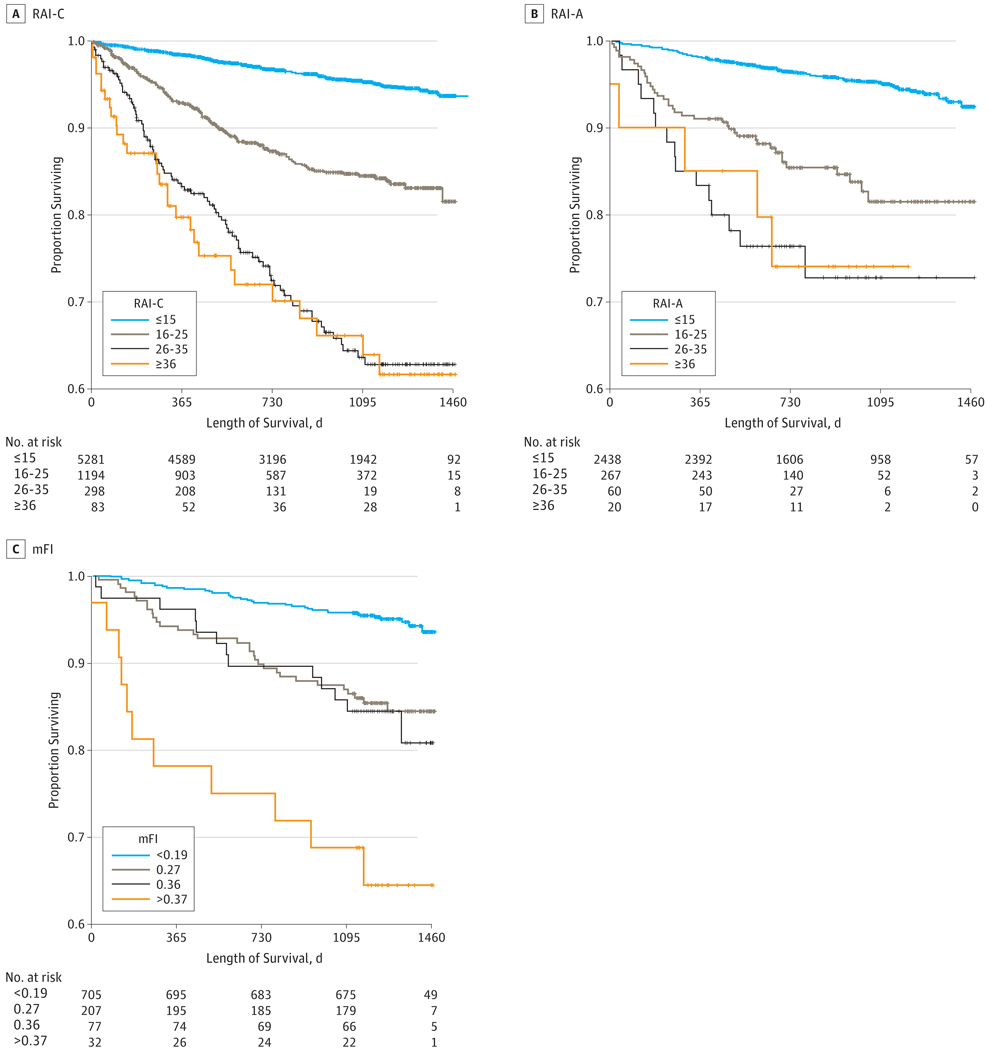
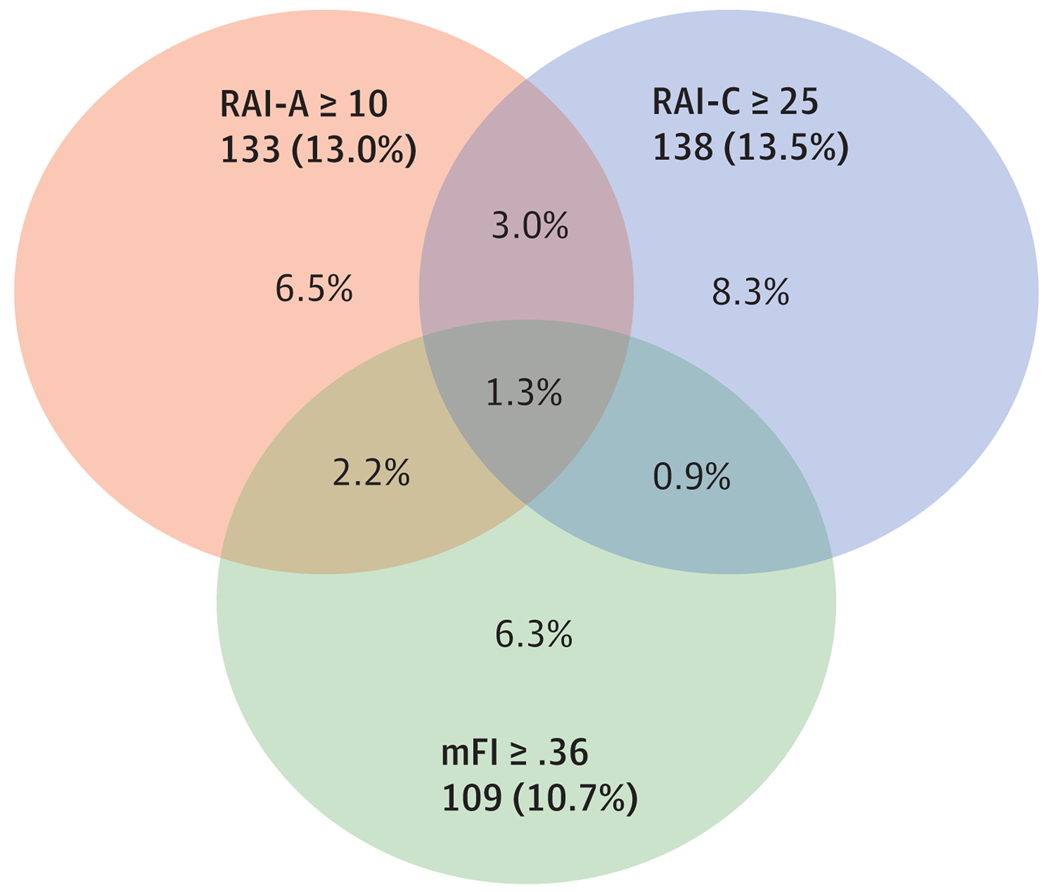
Results: Of the participants, the mean (SD) age was 60.7 (13.9) years and 249 participants (3.6%) were women. We assessed the RAI-C 10 698 times, from which we linked 6856 unique patients to mortality data. The C statistic predicting 180-day mortality for the RAI-C was 0.772. Of these 6856 unique patients, we linked 2785 to local Veterans Affairs Surgeons National Surgical Quality Improvement Projects data and calculated the C statistic for both the RAI-A (0.823) and RAI-C (0.824), along with the correlation between the 2 scores (r = 0.478; P < .001). Of these 2785 patients, there were sufficient data to calculate the modified Frailty Index for 1021, in which the C statistics were 0.865 (RAI-A), 0.797 (RAI-C), and 0.811 (modified Frailty Index). The correlation between the RAI-A and RAI-C was 0.547, and the correlations of the modified Frailty Index to the RAI-A and RAI-C were 0.301 and 0.269, respectively (all P < .001). A cutoff of RAI-C of at least 21 classified 18.3% patients as "frail" with a sensitivity of 0.50 and specificity of 0.82, whereas the RAI-A was less sensitive (0.25) and more specific (0.97), classifying only 3.7% as "frail."
Conclusions and relevance: The RAI-C and RAI-A represent effective tools for measuring frailty in surgical populations with predictive ability on par with other frailty tools. Moderate correlation between the measures suggests convergent validity. The RAI-C offers the advantage of prospective, preoperative assessment that is proved feasible for large-scale screening in clinical practice. However, further efforts should be directed at determining the optimal components of preoperative frailty assessment.
Conflict of interest statement
Figures
Comment in
-
Preoperative frailty status measured by Clinical Risk Analysis Index and adverse events after endoscopic endonasal transsphenoidal resection of pituitary adenoma: results of a single center prospective case series.J Neurosurg Sci. 2023 Aug;67(4):539-541. doi: 10.23736/S0390-5616.22.05947-1. Epub 2023 Jan 24. J Neurosurg Sci. 2023. PMID: 36692309 No abstract available.
References
-
- Sternberg SA, Wershof Schwartz A, Karunananthan S, Bergman H, Mark Clarfield A. The identification of frailty: a systematic literature review. J Am Geriatr Soc. 2011;59(11):2129–2138. - PubMed
-
- Fried LP, Ferrucci L, Darer J, Williamson JD, Anderson G. Untangling the concepts of disability, frailty, and comorbidity: implications for improved targeting and care. J Gerontol A Biol Sci Med Sci. 2004;59(3):255–263. - PubMed
-
- Fried LP, Tangen CM, Walston J, et al.; Cardiovascular Health Study Collaborative Research Group. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. 2001;56 (3):M146–M156. - PubMed
-
- Rockwood K, Mitnitski A. Frailty defined by deficit accumulation and geriatric medicine defined by frailty. Clin Geriatr Med. 2011;27(1):17–26. - PubMed
-
- Dayhoff NE, Suhrheinrich J, Wigglesworth J, Topp R, Moore S. Balance and muscle strength as predictors of frailty among older adults. J Gerontol Nurs. 1998;24(7):18–27. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
