

High-risk HPV genotypes and P16INK4a expression in a cohort of head and neck squamous cell carcinoma patients in Singapore
- PMID: 27893418
- PMCID: PMC5349949
- DOI: 10.18632/oncotarget.13502
High-risk HPV genotypes and P16INK4a expression in a cohort of head and neck squamous cell carcinoma patients in Singapore
Abstract
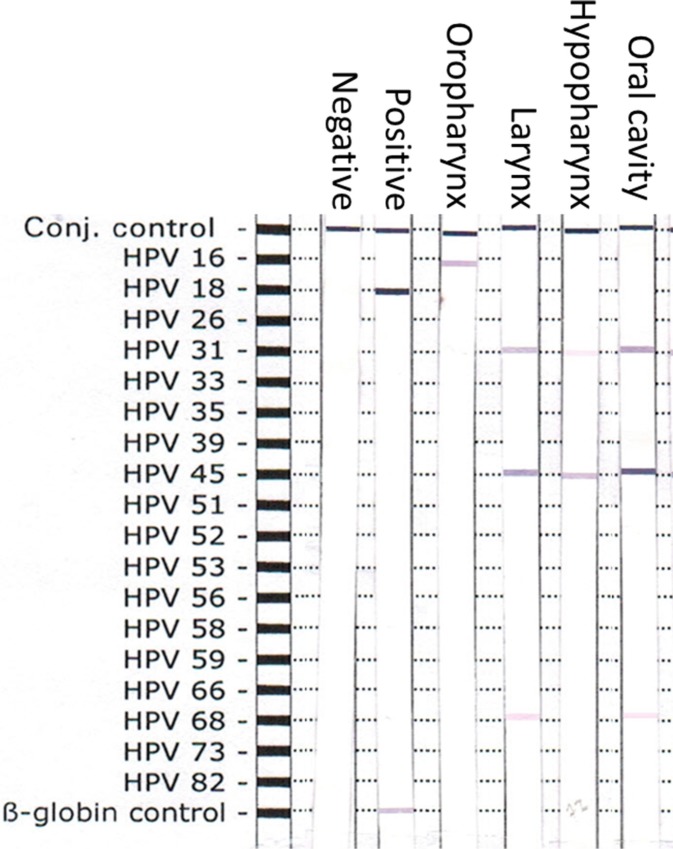
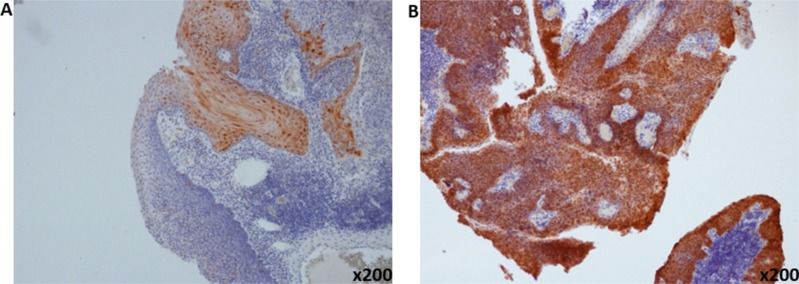
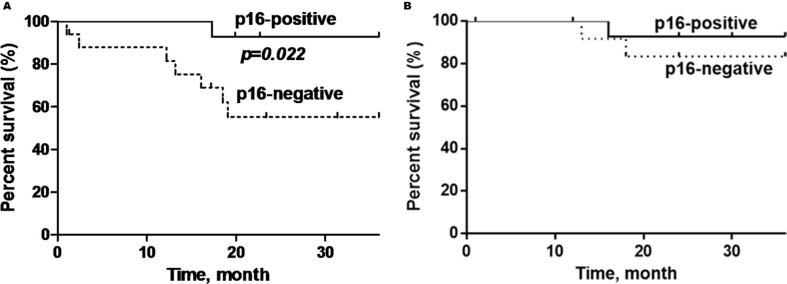
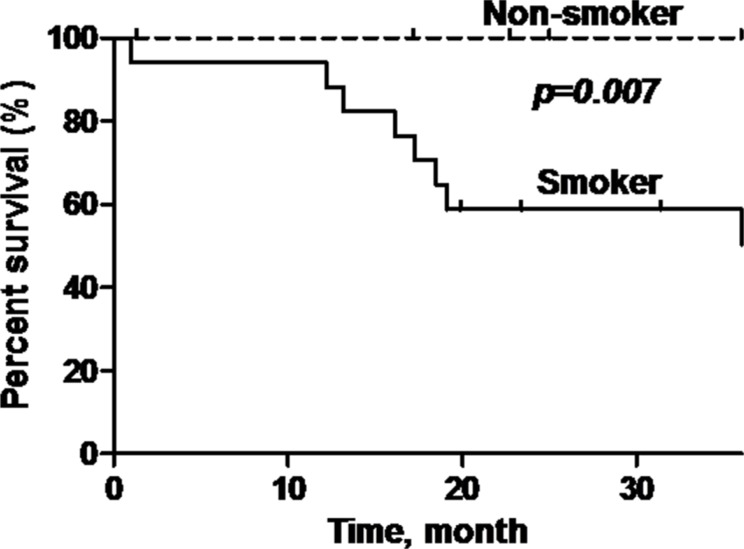
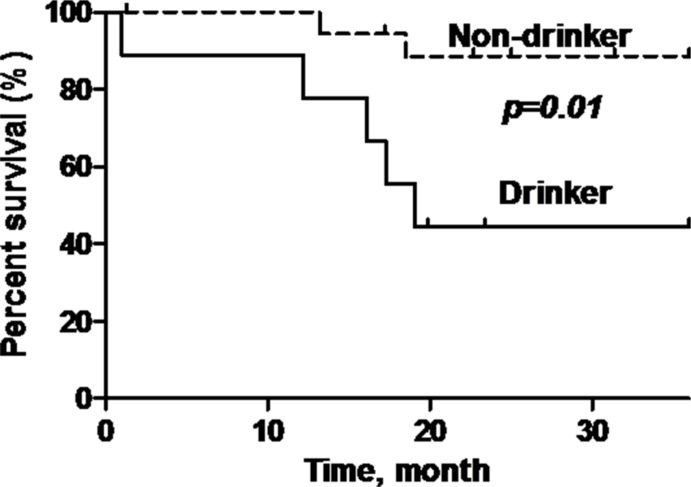
Human papillomavirus (HPV), especially HPV16 genotype, is associated with oropharyngeal squamous cell carcinoma (OPSCC). We aim to determine the prevalence and characterize the high-risk (HR)-HPV genotypes in head and neck SCC (HNSCC) in a South-East Asian multi-ethnic society in Singapore and examine its prognostic significance.159 HNSCC archival tissue samples were retrieved and tumour DNA was screened for 18 HR-HPV genotypes using a PCR-based assay (Qiagen, digene HPV genotyping RH test). P16 protein overexpression was identified using immunohistochemistry (IHC). Statistical correlation between clinical outcomes were performed between HPV-positive and negative HNSCC patients.Six HR-HPVs (HPV16, 18, 31, 45, 56, 68) were detected in 90.6% of HNSCC; and 79.9% had multiple HPV genotypes detected. HPV31 and HPV45 were the most prevalent (79.2% and 87.4%, respectively); and HPV16 was predominantly found in OPSCC (p < 0.001). HPV-DNA PCR assay yielded a high sensitivity (96%) but low specificity (11%) when compared to p16 immunohistochemistry as the reference standard.P16-positive HNSCC was predominantly observed in OPSCC (73.7%; p = 0.005); and p16-positive OPSCC exhibited improved overall survival compared to p16-negative OPSCC (p = 0.022). Similarly, smoking and alcohol consumption were poor prognostic factors of overall survival (p = 0.007; p = 0.01) in OPSCC patients.HR-HPVs were identified in 90.6% of HNSCC patients using the HPV-DNA PCR assay. This test had a poor specificity when compared to p16 IHC; making it an unreliable detection technique in selecting patients for radiation dose de-escalation treatment protocol. P16-positive tumor was predominantly found in the oropharynx these patients demonstrated better overall survival than those with p16-negative OPSCC.
Keywords: HPV DNA; head and neck squamous cell carcinoma; human papillomavirus; oropharyngeal squamous cell carcinoma; p16 immunohistochemistry.
Conflict of interest statement
None.
Figures
References
-
- Haraf DJ, Nodzenski E, Brachman D, Mick R, Montag A, Graves D, Vokes EE, Weichselbaum RR. Human papilloma virus and p53 in head and neck cancer: clinical correlates and survival. Clin Cancer Res. 1996;2:755–762. - PubMed
-
- Gillison ML, Koch WM, Capone RB, Spafford M, Westra WH, Wu L, Zahurak ML, Daniel RW, Viglione M, Symer DE, Shah KV, Sidransky D. Evidence for a causal association between human papillomavirus and a subset of head and neck cancers. J Natl Cancer Inst. 2000;92:709–720. - PubMed
-
- Munoz N, Bosch FX, de Sanjose S, Herrero R, Castellsague X, Shah KV, Snijders PJ, Meijer CJ. International Agency for Research on Cancer Multicenter Cervical Cancer Study G. Epidemiologic classification of human papillomavirus types associated with cervical cancer. N Engl J Med. 2003;348:518–527. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
