

T Cell Receptor Vβ Staining Identifies the Malignant Clone in Adult T cell Leukemia and Reveals Killing of Leukemia Cells by Autologous CD8+ T cells
- PMID: 27893842
- PMCID: PMC5125714
- DOI: 10.1371/journal.ppat.1006030
T Cell Receptor Vβ Staining Identifies the Malignant Clone in Adult T cell Leukemia and Reveals Killing of Leukemia Cells by Autologous CD8+ T cells
Abstract
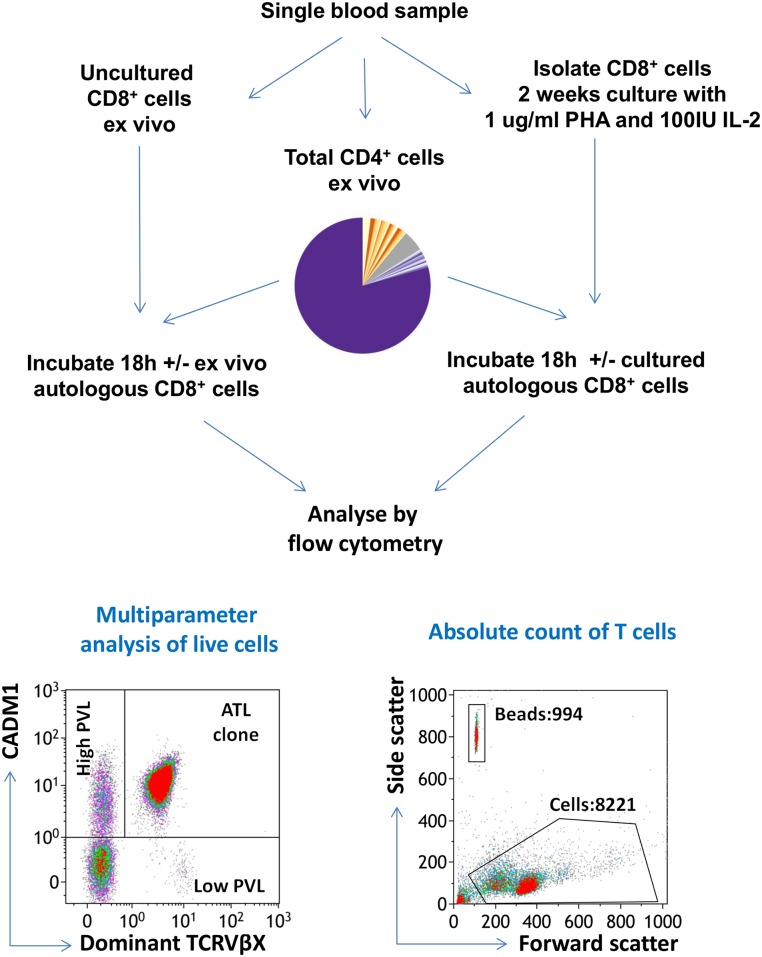
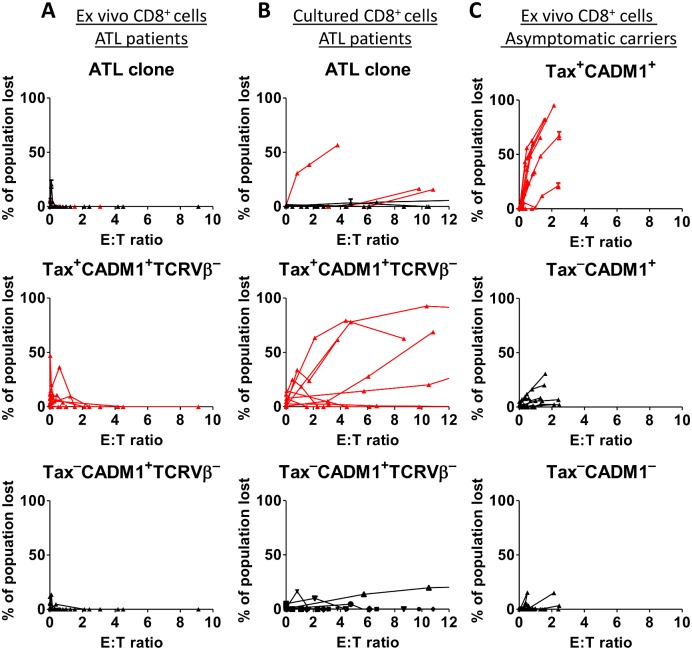
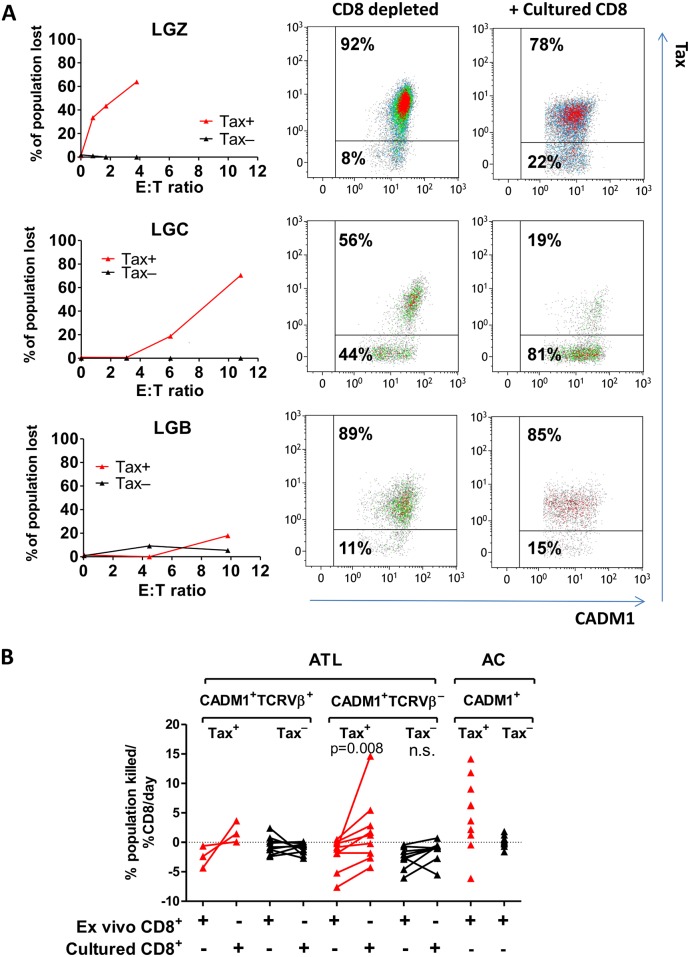
There is growing evidence that CD8+ cytotoxic T lymphocyte (CTL) responses can contribute to long-term remission of many malignancies. The etiological agent of adult T-cell leukemia/lymphoma (ATL), human T lymphotropic virus type-1 (HTLV-1), contains highly immunogenic CTL epitopes, but ATL patients typically have low frequencies of cytokine-producing HTLV-1-specific CD8+ cells in the circulation. It remains unclear whether patients with ATL possess CTLs that can kill the malignant HTLV-1 infected clone. Here we used flow cytometric staining of TCRVβ and cell adhesion molecule-1 (CADM1) to identify monoclonal populations of HTLV-1-infected T cells in the peripheral blood of patients with ATL. Thus, we quantified the rate of CD8+-mediated killing of the putative malignant clone in ex vivo blood samples. We observed that CD8+ cells from ATL patients were unable to lyse autologous ATL clones when tested directly ex vivo. However, short in vitro culture restored the ability of CD8+ cells to kill ex vivo ATL clones in some donors. The capacity of CD8+ cells to lyse HTLV-1 infected cells which expressed the viral sense strand gene products was significantly enhanced after in vitro culture, and donors with an ATL clone that expressed the HTLV-1 Tax gene were most likely to make a detectable lytic CD8+ response to the ATL cells. We conclude that some patients with ATL possess functional tumour-specific CTLs which could be exploited to contribute to control of the disease.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Shimoyama M. Diagnostic criteria and classification of clinical subtypes of adult T-cell leukaemia-lymphoma. A report from the Lymphoma Study Group (1984–87). Br J Haematol. 1991;79: 428–437. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
