

Can morphological MRI differentiate between primary central nervous system lymphoma and glioblastoma?
- PMID: 27894359
- PMCID: PMC5126849
- DOI: 10.1186/s40644-016-0098-9
Can morphological MRI differentiate between primary central nervous system lymphoma and glioblastoma?
Abstract
Background: Primary central nervous system lymphoma (PCNSL) is a rare, aggressive brain neoplasm that accounts for roughly 2-6% of primary brain tumors. In contrast, glioblastoma (GBM) is the most frequent and severe glioma subtype, accounting for approximately 50% of diffuse gliomas. The aim of the present study was to evaluate morphological MRI characteristics in histologically-proven PCNSL and GBM at the time of their initial presentation.
Methods: We retrospectively evaluated standard diagnostic MRI examinations in 54 immunocompetent patients (26 female, 28 male; age 62.6 ± 11.5 years) with histologically-proven PCNSL and 54 GBM subjects (21 female, 33 male; age 59 ± 14 years).
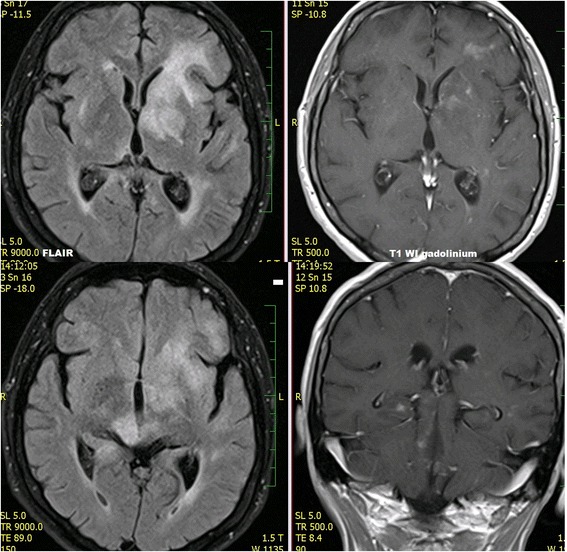
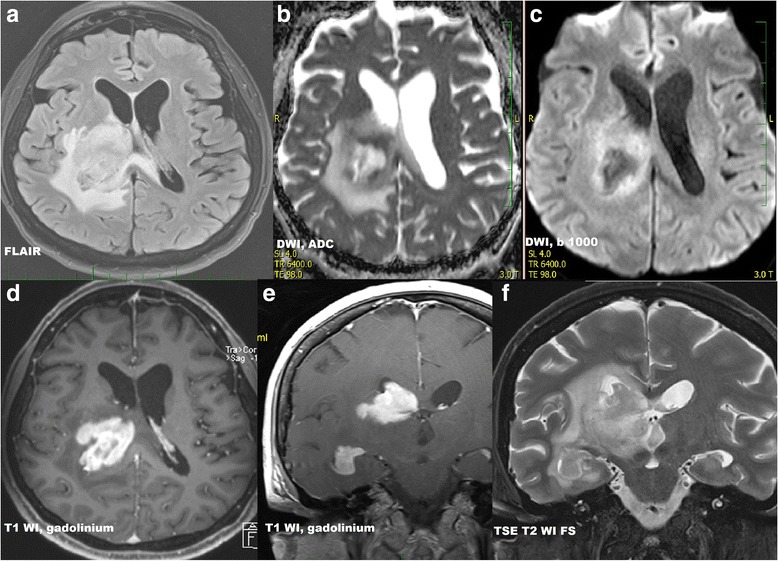
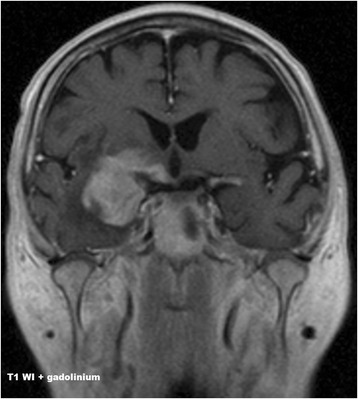
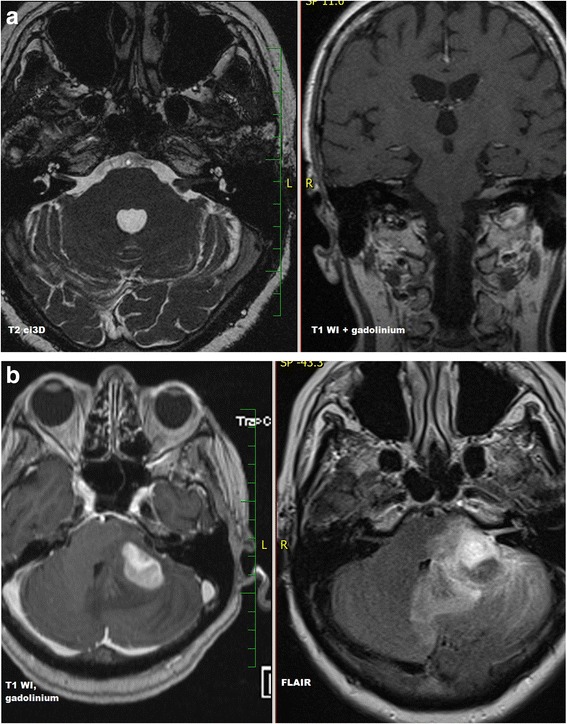
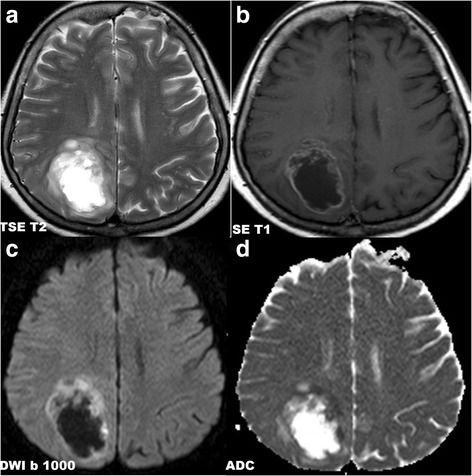
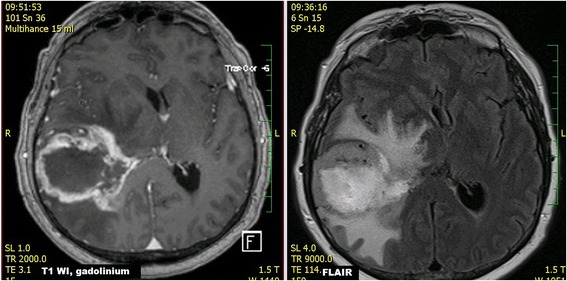
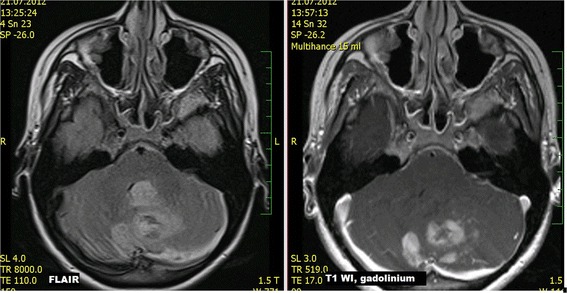
Results: Several significant differences between both infiltrative brain tumors were found. PCNSL lesions enhanced homogenously in 64.8% of cases, while nonhomogeneous enhancement was observed in 98.1% of GBM cases. Necrosis was present in 88.9% of GBM lesions and only 5.6% of PCNSL lesions. PCNSL presented as multiple lesions in 51.9% cases and in 35.2% of GBM cases; however, diffuse infiltrative type of brain involvement was observed only in PCNSL (24.1%). Optic pathways were infiltrated more commonly in PCNSL than in GBM (42.6% vs. 5.6%, respectively, p <0.001). Other cranial nerves were affected in 5.6% of PCNSL, and in none of GBM. Signs of bleeding were rare in PCNSL (5.6%) and common in GBM (44.4%); p < 0.001. Both supratentorial and infratentorial localization was present only in PCNSL (27.7%). Involvement of the basal ganglia was more common in PCNSL (55.6%) than in GBM (18.5%); (p < 0.001). Cerebral cortex was affected significantly more often in GBM (83.3%) than in PCNSL (51.9%); mostly by both enhancing and non-enhancing infiltration.
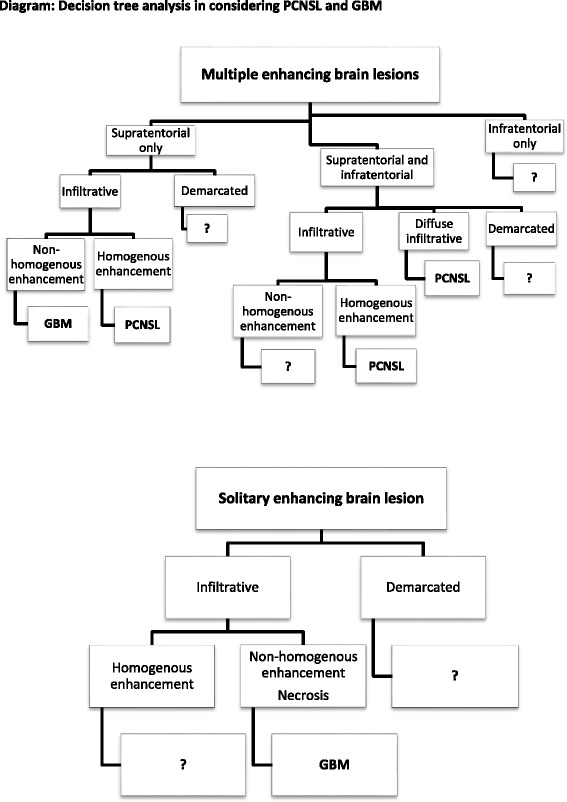
Conclusion: Routine morphological MRI is capable of differentiating between GBM and PCNSL lesions in many cases at time of initial presentation. A solitary infiltrative supratentorial lesion with nonhomogeneous enhancement and necrosis was typical for GBM. PCNSL presented with multiple lesions that enhanced homogenously or as diffuse infiltrative type of brain involvement, often with basal ganglia and optic pathways affection.
Keywords: Conventional MRI; Enhancement; Initial evaluation.
Figures
References
-
- van der Sanden GA, Schouten LJ, van Dijck JA, van Andel JP, van der Maazen RW, Coebergh JW, Working Group of Specialists in Neuro-Oncology in the Southern and Eastern Netherlands Primary central system lymphomas: incidence and survival in the Southern and Eastern Netherlands. Cancer. 2002;94(5):1547–56. - PubMed
-
- Bhagavathi S, Wilson JD. Primary central nervous system lymphoma. Arch Pathol Lab Med. 2008;132(11):1830–1834. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
