

Optimal Fluid Therapy for Traumatic Hemorrhagic Shock
- PMID: 27894494
- PMCID: PMC5131713
- DOI: 10.1016/j.ccc.2016.08.007
Optimal Fluid Therapy for Traumatic Hemorrhagic Shock
Abstract
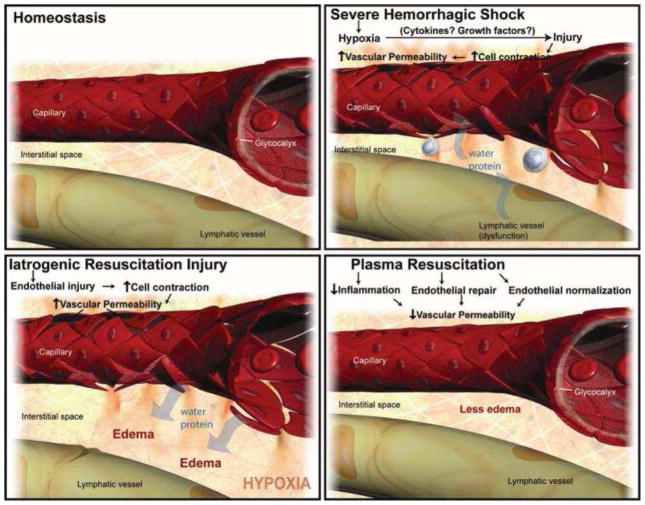
The resuscitation of traumatic hemorrhagic shock has undergone a paradigm shift in the last 20 years with the advent of damage control resuscitation (DCR). Major principles of DCR include minimization of crystalloid, permissive hypotension, transfusion of a balanced ratio of blood products, and goal-directed correction of coagulopathy. In particular, plasma has replaced crystalloid as the primary means for volume expansion for traumatic hemorrhagic shock. Predicting which patient will require DCR by prompt and accurate activation of a massive transfusion protocol, however, remains a challenge.
Keywords: Damage control resuscitation; Hemorrhagic shock; Massive transfusion protocol.
Copyright © 2016 Elsevier Inc. All rights reserved.
Conflict of interest statement
No relevant financial conflicts of interest.
Figures
References
-
- Tien HC, Spencer F, Tremblay LN, et al. Preventable deaths from hemorrhage at a level I Canadian trauma center. J Trauma. 2007;62:142–146. - PubMed
-
- Sauaia A, Moore FA, Moore EE, et al. Epidemiology of trauma deaths: a reassessment. J Trauma. 1995;38:185–193. - PubMed
-
- Eastridge BJ, Malone D, Holcomb JB. Early predictors of transfusion and mortality after injury: A review of the data-based literature. J Trauma. 2006;60(6 Suppl):S20–S25. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
