

Optimal Computed Tomographic Perfusion Scan Duration for Assessment of Acute Stroke Lesion Volumes
- PMID: 27895299
- PMCID: PMC5134896
- DOI: 10.1161/STROKEAHA.116.014177
Optimal Computed Tomographic Perfusion Scan Duration for Assessment of Acute Stroke Lesion Volumes
Abstract
Background and purpose: The minimal scan duration needed to obtain reliable lesion volumes with computed tomographic perfusion (CTP) has not been well established in the literature.
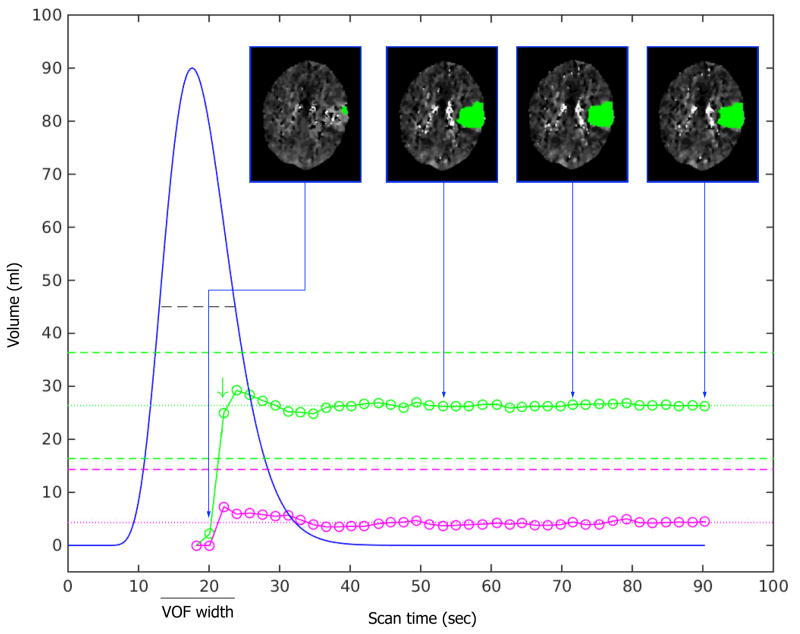
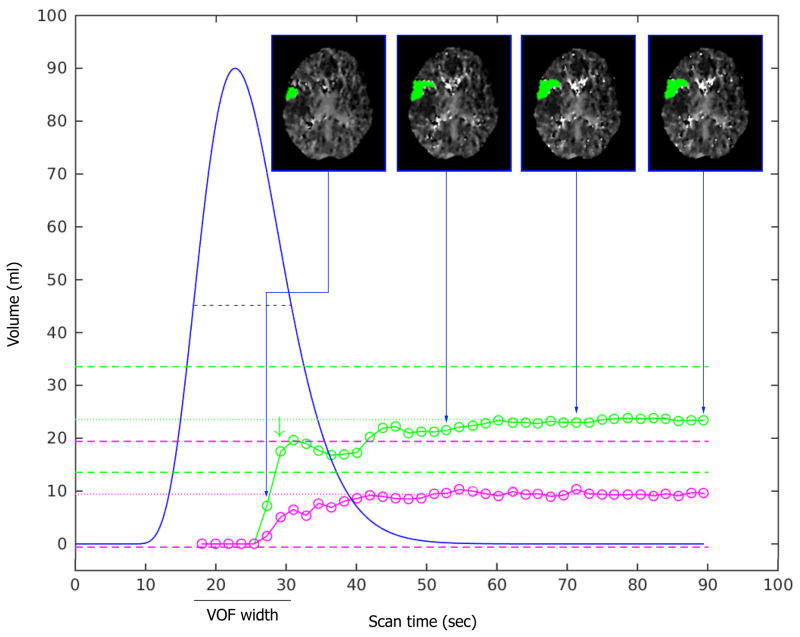
Methods: We retrospectively assessed the impact of gradual truncation of the scan duration on acute ischemic lesion volume measurements. For each scan, we identified its optimal scan time, defined as the shortest scan duration that yields measurements of the ischemic lesion volumes similar to those obtained with longer scanning, and the relative height of the fitted venous output function at its optimal scan time.
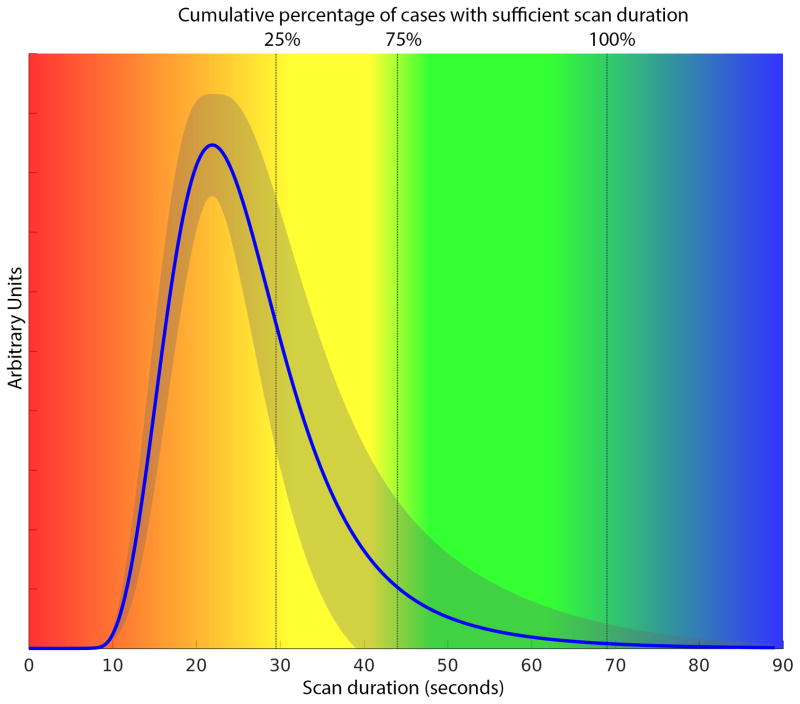
Results: We analyzed 70 computed tomographic perfusion scans of acute stroke patients. An optimal scan time could not be determined in 11 scans (16%). For the other 59 scans, the median optimal scan time was 32.7 seconds (90th percentile 52.6 seconds; 100th percentile 68.9 seconds), and the median relative height of the fitted venous output function at the optimal scan times was 0.39 (90th percentile 0.02; 100th percentile 0.00). On the basis of a linear model, the optimal scan time was T0 plus 1.6 times the width of the venous output function (P<0.001; R2=0.49).
Conclusions: This study shows how the optimal duration of a computed tomographic perfusion scan relates to the arrival time and width of the contrast bolus. This knowledge can be used to optimize computed tomographic perfusion scan protocols and to determine whether a scan is of sufficient duration. Provided a baseline (T0) of 10 seconds, a total scan duration of 60 to 70 seconds, which includes the entire downslope of the venous output function in most patients, is recommended.
Keywords: magnetic resonance imaging; perfusion imaging; reperfusion; stroke.
© 2016 American Heart Association, Inc.
Conflict of interest statement
DISCLOSURES/CONFLICT OF INTEREST G. Albers has received consulting fees and expenses from Lundbeck for Steering Committee work and consulting fees from Concentric for serving on a Data Safely and Monitory Board. G Albers and R Bammer are equity shareholders in iSchemaView and perform consulting work for iSchemaView. Soren Christensen performs consulting work for iSchemaView. All other authors report no conflicts of interest.
Figures
References
-
- Heiss WD, Sobesky J, Hesselmann V. Identifying thresholds for penumbra and irreversible tissue damage. Stroke. 2004;35:2671–4. - PubMed
-
- Wintermark M, Flanders AE, Velthuis B, Meuli R, van LM, Goldsher D, et al. Perfusion-CT assessment of infarct core and penumbra: receiver operating characteristic curve analysis in 130 patients suspected of acute hemispheric stroke. Stroke. 2006;37:979–85. - PubMed
-
- Bivard A, Spratt N, Levi C, Parsons M. Perfusion computer tomography: imaging and clinical validation in acute ischaemic stroke. Brain. 2011;134:3408–16. - PubMed
-
- Campbell BC, Christensen S, Levi CR, Desmond PM, Donnan GA, Davis SM, et al. Cerebral blood flow is the optimal CT perfusion parameter for assessing infarct core. Stroke. 2011;42:3435–40. - PubMed
-
- Campbell BC, Mitchell PJ, Kleinig TJ, Dewey HM, Churilov L, Yassi N, et al. Endovascular therapy for ischemic stroke with perfusion-imaging selection. N Engl J Med. 2015;372:1009–18. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
