

Efficacy and safety of talimogene laherparepvec versus granulocyte-macrophage colony-stimulating factor in patients with stage IIIB/C and IVM1a melanoma: subanalysis of the Phase III OPTiM trial
- PMID: 27895500
- PMCID: PMC5119624
- DOI: 10.2147/OTT.S115245
Efficacy and safety of talimogene laherparepvec versus granulocyte-macrophage colony-stimulating factor in patients with stage IIIB/C and IVM1a melanoma: subanalysis of the Phase III OPTiM trial
Abstract
Objectives: Talimogene laherparepvec is the first oncolytic immunotherapy to receive approval in Europe, the USA and Australia. In the randomized, open-label Phase III OPTiM trial (NCT00769704), talimogene laherparepvec significantly improved durable response rate (DRR) versus granulocyte-macrophage colony-stimulating factor (GM-CSF) in 436 patients with unresectable stage IIIB-IVM1c melanoma. The median overall survival (OS) was longer versus GM-CSF in patients with earlier-stage melanoma (IIIB-IVM1a). Here, we report a detailed subgroup analysis of the OPTiM study in patients with IIIB-IVM1a disease.
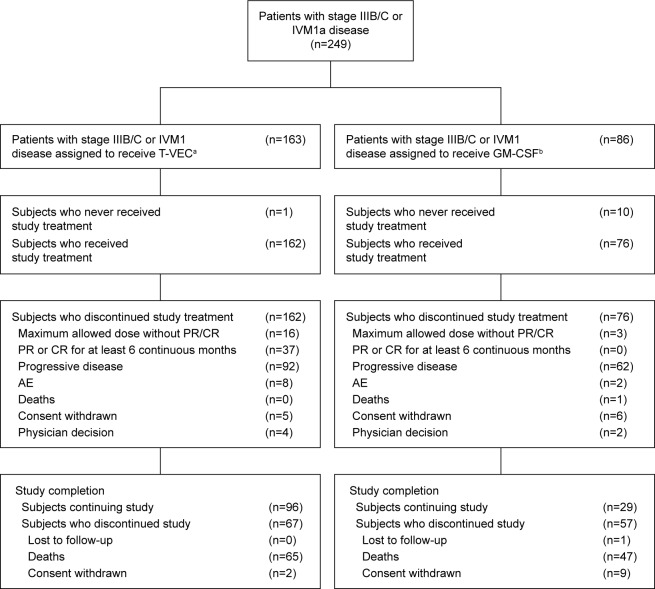
Patients and methods: The patients were randomized (2:1 ratio) to intralesional talimogene laherparepvec or subcutaneous GM-CSF and were evaluated for DRR, overall response rate (ORR), OS, safety, benefit-risk and numbers needed to treat. Descriptive statistics were used for subgroup comparisons.
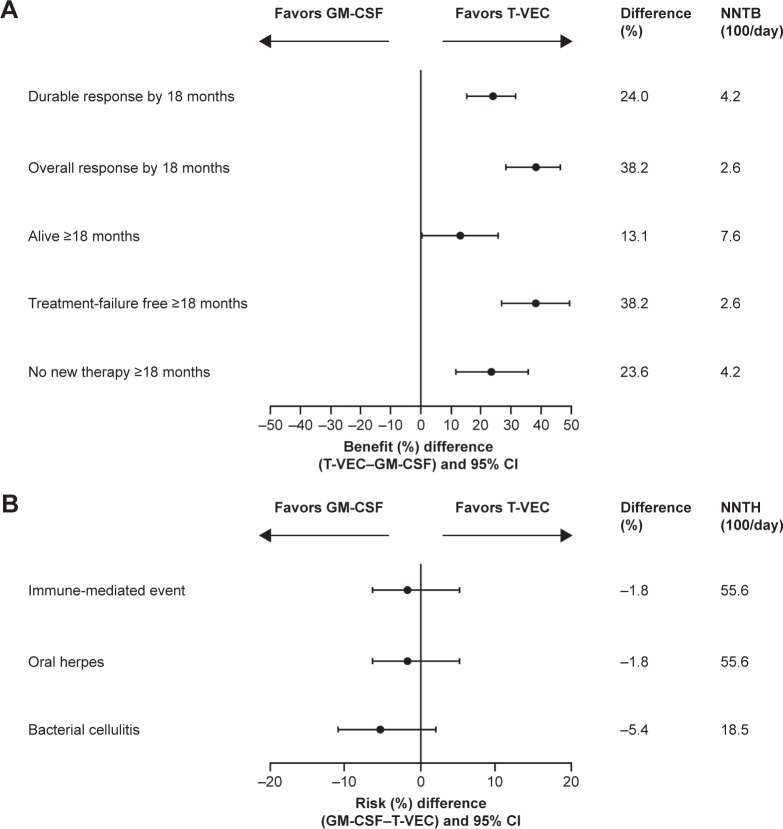
Results: Among 249 evaluated patients with stage IIIB-IVM1a melanoma, DRR was higher with talimogene laherparepvec compared with GM-CSF (25.2% versus 1.2%; P<0.0001). ORR was also higher in the talimogene laherparepvec arm (40.5% versus 2.3%; P<0.0001), and 27 patients in the talimogene laherparepvec arm had a complete response, compared with none in GM-CSF-treated patients. The incidence rates of exposure-adjusted adverse events (AE) and serious AEs were similar with both treatments.
Conclusion: The subgroup of patients with stage IIIB, IIIC and IVM1a melanoma (57.1% of the OPTiM intent-to-treat population) derived greater benefit in DRR and ORR from talimogene laherparepvec compared with GM-CSF. Talimogene laherparepvec was well tolerated.
Keywords: benefit–risk; clinical trial; durable response rate; immunotherapy; oncolytic virus; talimogene laherparepvec.
Conflict of interest statement
Kevin J Harrington discloses membership of scientific advisory boards for Amgen, AstraZeneca, Bristol Myers Squibb, Merck Sharp & Dohme, Pfizer and Viralytics and discloses a consulting role with Amgen, AstraZeneca, Bristol Myers Squibb, Merck Sharp & Dohme, Pfizer and Viralytics. Kevin J Harrington acknowledges support from the The Institute of Cancer Research/The Royal Marsden Hospital NIHR Biomedical Research Centre. Robert HI Andtbacka discloses a consulting role with Amgen. Frances Collichio discloses a consulting role with Amgen; the University of North Carolina School of Medicine receives clinical trials funding from Amgen. Gerald Downey, Lisa Chen and Zsolt Szabo are employees of Amgen. Howard L Kaufman discloses membership of scientific advisory boards for Alkermes, Amgen, EMD Serono, Merck, Prometheus and Sanofi and involvement in a speaker’s bureau for Merck. The authors report no other conflicts of interest in this work.
Figures
References
-
- United States Food and Drug Administration [webpage on the Internet] Food and Drug Administration (FDA) Approves First-of-Its-Kind Product for the Treatment of Melanoma. 2015. [Accessed December 1, 2015]. Available from: http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm469571.htm.
-
- European Medicines Agency The Committee for Medicinal Products for Human Use (CHMP) Summary of Opinion for Imlygic. 2015. [Accessed December 1, 2015]. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/Summary_of_opinion_....
-
- Ledford H. Cancer-fighting viruses win approval. Nature. 2015;526(7575):622–623. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
