

Rectal separation using hydroxypropyl methylcellulose in intracavitary brachytherapy of cervical cancer: an innovative approach
- PMID: 27895681
- PMCID: PMC5116447
- DOI: 10.5114/jcb.2016.62951
Rectal separation using hydroxypropyl methylcellulose in intracavitary brachytherapy of cervical cancer: an innovative approach
Abstract
Purpose: This study was initiated to prove feasibility of hydrogel application in recto-vaginal space in intracavitary brachytherapy (ICBT) of cervical cancer in order to reduce rectal toxicity.
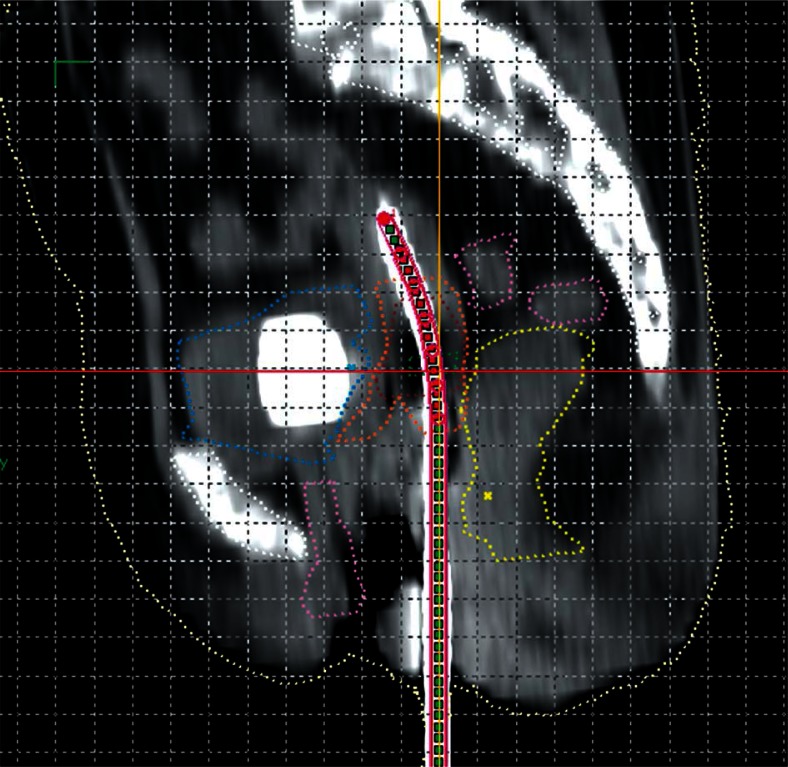
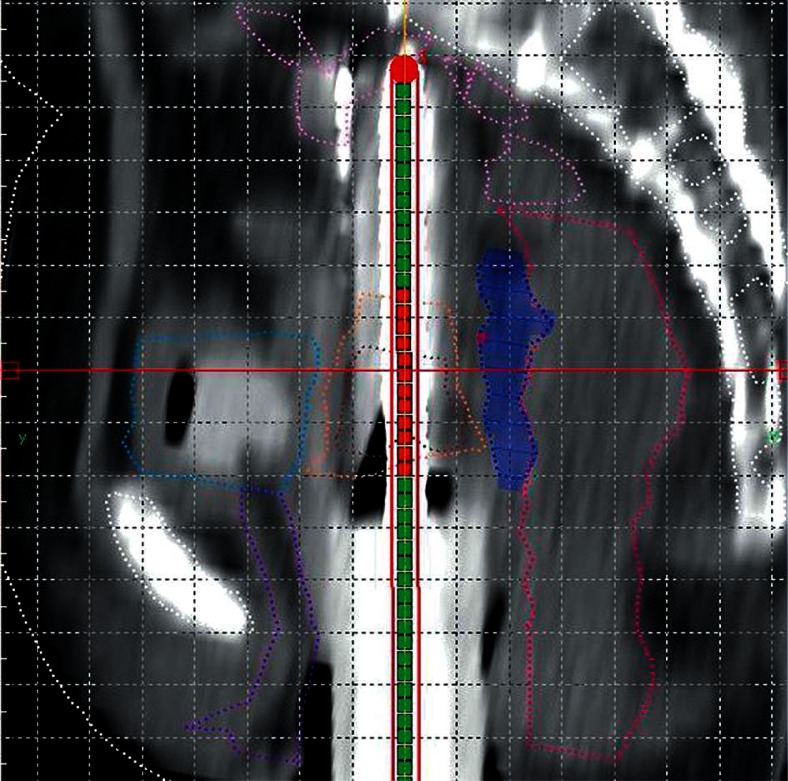
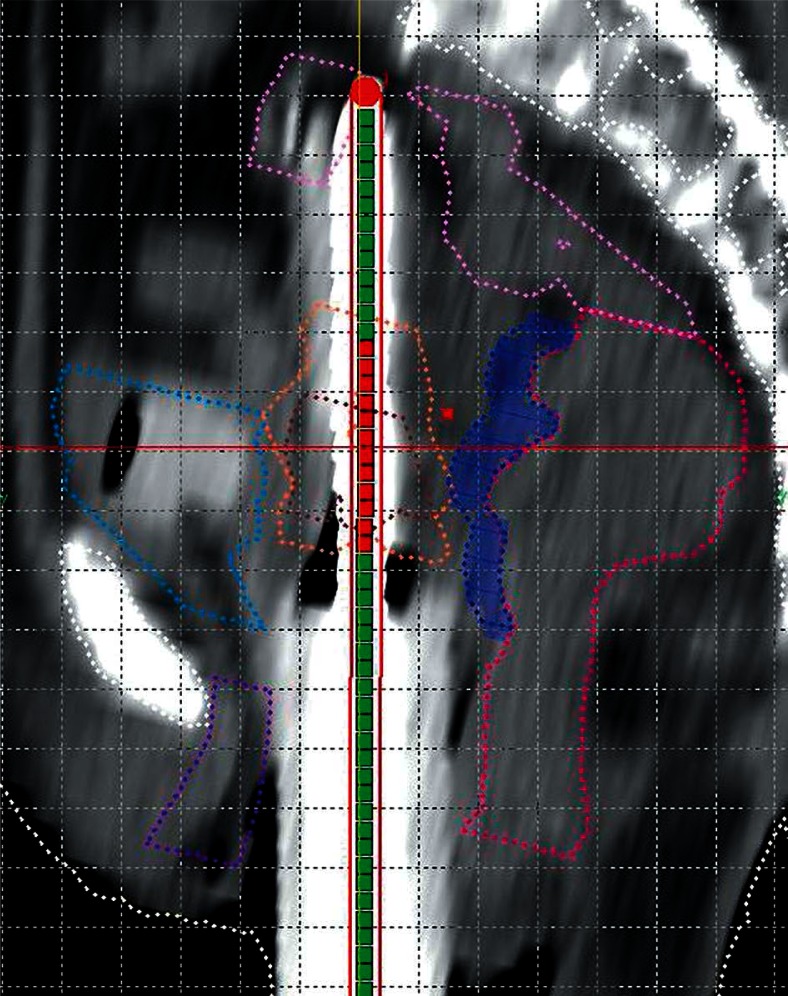
Material and methods: In a case of stage IIB cervical cancer, after external beam radiotherapy (EBRT), we planned ICBT 7 Gy × 3 fractions. In 1st fraction (Plan 1), due to narrow separation between rectum and cervix (0.18 cm), only 5 Gy was delivered at point A (with high-risk clinical target volume [HR-CTV] D90 5.94 Gy, intermediate risk clinical target volume [IR-CTV] D90 4.54 Gy, rectum D2cc 5.72 Gy, bladder D2cc 5.52 Gy, and sigmoid colon 5.82 Gy). In 2nd fraction (Plan 2), interstitial brachytherapy (ISBT) was attempted. For the prescription of 5 Gy, we get dose levels almost similar to the 1st insertion: HR-CTV D90 (6.7 Gy), IR-CTV D90 (3.06 Gy), bladder D2cc (5.7 Gy), rectum D2cc (4.8 Gy), sigmoid colon D2cc (1.3 Gy) (separation = 0.23 cm). During 3rd fraction (Plan 3), prior doing interstitial insertion, we instilled 50 cc of hydroxypropyl methylcellulose (Viscomet®) up to the tip of recto-vaginal septum. A repeat computed tomography (CT) scan was done 4 hours after Plan 3 treatment and it was re-planned (Plan 4) to find out migration of hydrogel if any and its dosimetric impact.
Results: 9 Gy was delivered to point A with a separation of 1.1 cm in Plan 3 (with HR-CTV D90 16.4 Gy, IR-CTV D90 11.3 Gy, rectum D2cc 3.6 Gy, bladder D2cc 6.9 Gy, and sigmoid colon 2.2 Gy). We achieved an optimum cumulative EQD2 dose (HR-CTV D90 98.4 Gy, IR-CTV D90 76.1 Gy, rectum D2cc 67.7 Gy, bladder D2cc 73.2 Gy, and sigmoid colon 59.3 Gy). Hydrogel volume was decreased in Plan 4 without a major dosimetric changes.
Conclusions: Hydrogel instillation is a useful tool for recto-vaginal separation during cervical cancer brachytherapy. It increases therapeutic ratio without any adverse event.
Keywords: brachytherapy; cervical cancer; rectal toxicity.
Figures
References
-
- Barillot I, Horiot JC, Maingon P, et al. Impact on treatment outcome and late effects of customized treatment planning in cervix carcinomas: baseline results to compare new strategies. Int J Radiat Oncol Biol Phys. 2000;48:189–200. - PubMed
-
- Chen SW, Liang JA, Yang SN, et al. The prediction of late rectal complications following the treatment of uterine cervical cancer by high-dose-rate brachytherapy. Int J Radiat Oncol Biol Phys. 2000;47:955–961. - PubMed
-
- Eifel PJ, Thoms WW, Jr, Smith TL, et al. The relationship between brachytherapy dose and outcome in patients with bulky endocervical tumors treated with radiation alone. Int J Radiat Oncol Biol Phys. 1994;28:113–118. - PubMed
-
- Eifel PJ, Levenback C, Wharton T, et al. Time course and incidence of late complications in patients treated with radiation therapy for FIGO stage Ib carcinoma of the uterine cervix. Int J Radiat Oncol Biol Phys. 1995;32:1289–1300. - PubMed
-
- Perez CA, Grigsby PW, Lockett MA, et al. Radiation therapy morbidity in carcinoma of the uterine cervix: dosimetric and clinical correlation. Int J Radiat Oncol Biol Phys. 1999;44:855–866. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous