

Efficacy of a low-cost bubble CPAP system in treatment of respiratory distress in a neonatal ward in Malawi
- PMID: 27895847
- PMCID: PMC5117003
Efficacy of a low-cost bubble CPAP system in treatment of respiratory distress in a neonatal ward in Malawi
Abstract
Background: Respiratory failure is a leading cause of neonatal mortality in the developing world. Bubble continuous positive airway pressure (bCPAP) is a safe, effective intervention for infants with respiratory distress and is widely used in developed countries. Because of its high cost, bCPAP is not widely utilized in low-resource settings. We evaluated the performance of a new bCPAP system to treat severe respiratory distress in a low resource setting, comparing it to nasal oxygen therapy, the current standard of care.
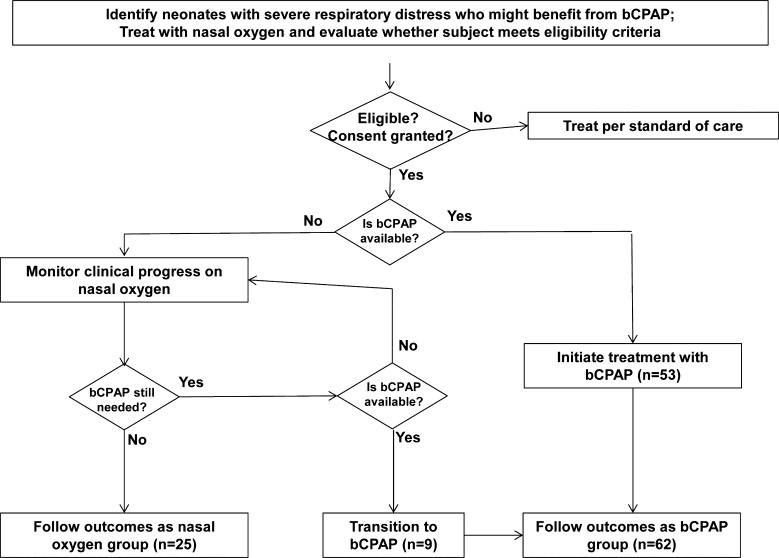
Methods: We conducted a non-randomized convenience sample study to test the efficacy of a low-cost bCPAP system treating newborns with severe respiratory distress in the neonatal ward of Queen Elizabeth Central Hospital, in Blantyre, Malawi. Neonates weighing >1,000 g and presenting with severe respiratory distress who fulfilled inclusion criteria received nasal bCPAP if a device was available; if not, they received standard care. Clinical assessments were made during treatment and outcomes compared for the two groups.
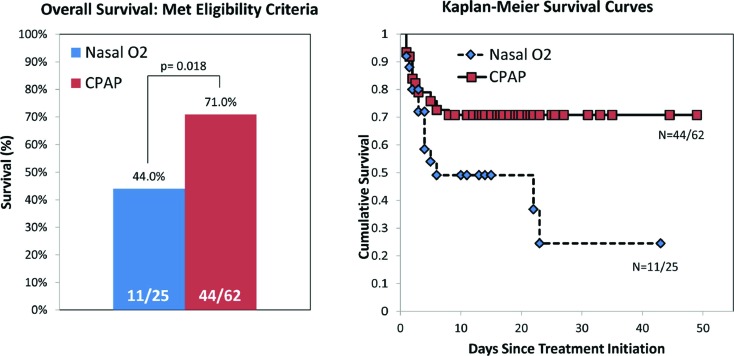
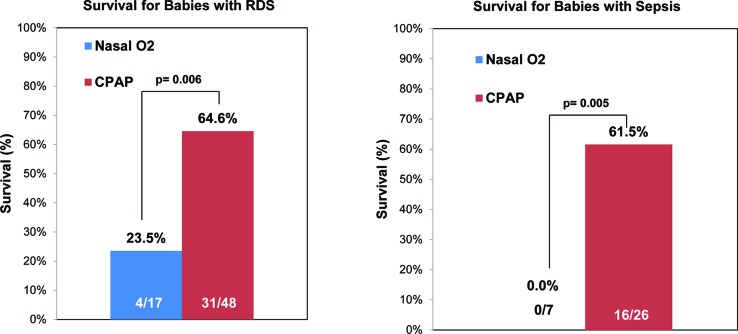
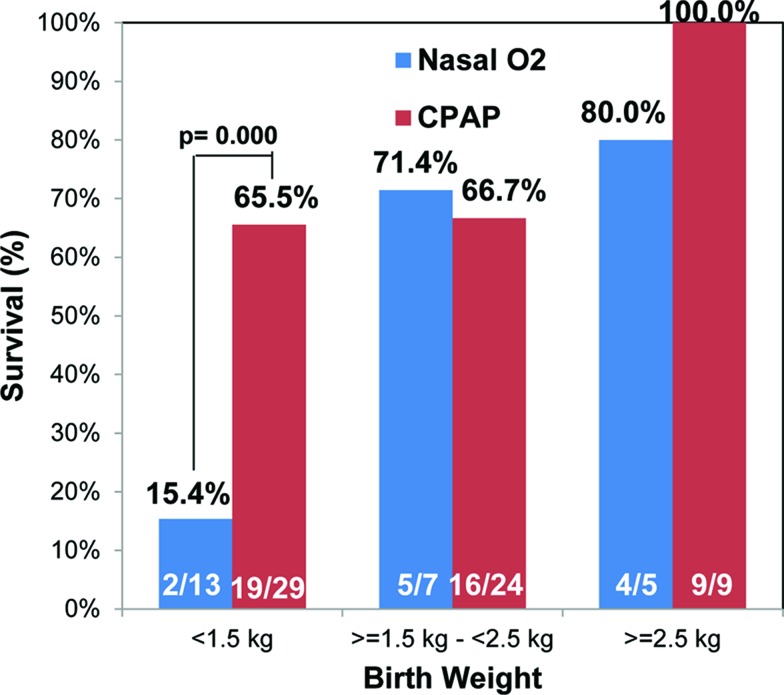
Findings: 87 neonates (62 bCPAP, 25 controls) were recruited. Survival rate for neonates receiving bCPAP was 71.0% (44/62) compared with 44.0% (11/25) for controls. 65.5% (19/29) of very low birth weight neonates receiving bCPAP survived to discharge compared to 15.4% (1/13) of controls. 64.6% (31/48) of neonates with respiratory distress syndrome (RDS) receiving bCPAP survived to discharge, compared to 23.5% (4/17) of controls. 61.5% (16/26) of neonates with sepsis receiving bCPAP survived to discharge, while none of the seven neonates with sepsis in the control group survived.
Interpretation: Use of a low-cost bCPAP system to treat neonatal respiratory distress resulted in 27% absolute improvement in survival. The beneficial effect was greater for neonates with very low birth weight, RDS, or sepsis. Implementing appropriate bCPAP devices could reduce neonatal mortality in developing countries.
Figures

Republished from
-
Efficacy of a low-cost bubble CPAP system in treatment of respiratory distress in a neonatal ward in Malawi.PLoS One. 2014 Jan 29;9(1):e86327. doi: 10.1371/journal.pone.0086327. eCollection 2014. PLoS One. 2014. PMID: 24489715 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources