

Under-five mortality among displaced populations in Meheba refugee camp, Zambia, 2008-2014
- PMID: 27895911
- PMCID: PMC5116855
- DOI: 10.1186/s13690-016-0161-9
Under-five mortality among displaced populations in Meheba refugee camp, Zambia, 2008-2014
Abstract
Background: Under-five mortality, which is the probability of a child dying before their fifth birthday, is of concern in Zambia as infant and child mortality rates are important social indicators. Displaced population in camps provide a basis for under-five mortality surveillance because detailed registration databases have been developed. Additionally, health data routinely collected on mortality allowed for a review of mortality trends and identification of correlating factors to under-five mortality. Literature suggests a number of factors that influence child mortality including biological, socio-econimic and environmental factors. However, while progress in reducing mortality is evident disparities in under-five mortality trends have been observed.
Methods: The study examined differential levels and trends of under-five mortality with correlating factors in Meheba refugee camp in Zambia which is presently in its post emergency phase. The retrospective cross-sectional study reviewed the ProGres and Health Information System (HIS) databases under-five mortality data for a seven (7) year period (2008-2014) and included all children aged less than five years in each year of review. STATA 12 (including Ordinary Least Squares Regression) and Microsoft Excel 2010 where used for data analysis and computation of findings.
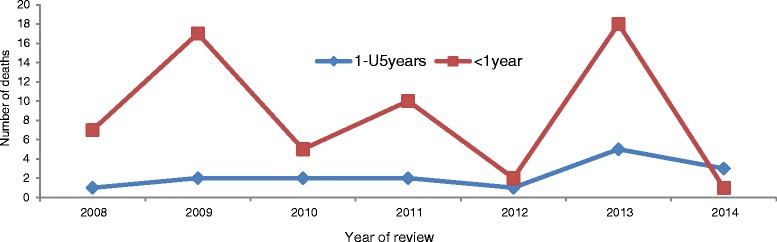
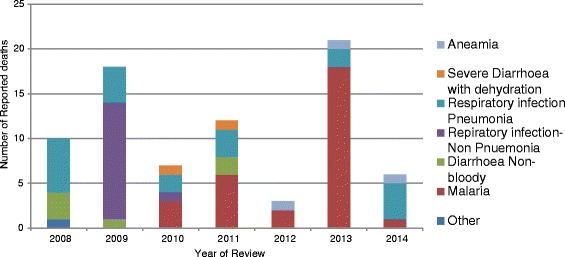
Results: Malaria and respiratory infections accounted for 81 % of under-five deaths while cases of Diarrhoea were responsible for 10 % of reported mortalities. Seventy five percent (75 %) of all mortalities were reported in children aged less than 1 year (<1 year). While no significant variations in mortality were noted as a result of time, increased frequency of visits to health centre significantly (P < 0.05) reduced mortalities in children by 3/1000 in each year.
Conclusion: In addition to improving health infrastructure and reducing distances to health facilities, the study also recommends sensitization programmes targeted at ensuring accessibility to health care services for children under-5 years. The study found that increased health centre visitations were associated with reduction in under-five mortality and encourages initiatives targeted at sensitizing communities to seek health care. Furthermore, collaboration between the health systems, community and Non Governmental Organisations (NGOs) is key in addressing higher infant mortality observed. It is envisaged that this will contribute to the reduction in mortality cases and will compliment already existing strategies.
Keywords: Displaced populations; Post emmergency phase; Refugee camps; Underfive mortality.
Figures



Similar articles
-
Famine-affected, refugee, and displaced populations: recommendations for public health issues.MMWR Recomm Rep. 1992 Jul 24;41(RR-13):1-76. MMWR Recomm Rep. 1992. PMID: 1326713
-
Incidence and risk factors for Malaria, pneumonia and diarrhea in children under 5 in UNHCR refugee camps: A retrospective study.Confl Health. 2011 Oct 26;5(1):24. doi: 10.1186/1752-1505-5-24. Confl Health. 2011. PMID: 22029694 Free PMC article.
-
Health programmes and policies associated with decreased mortality in displaced people in postemergency phase camps: a retrospective study.Lancet. 2002 Dec 14;360(9349):1927-34. doi: 10.1016/S0140-6736(02)11915-5. Lancet. 2002. PMID: 12493259
-
Italian cancer figures, report 2012: Cancer in children and adolescents.Epidemiol Prev. 2013 Jan-Feb;37(1 Suppl 1):1-225. Epidemiol Prev. 2013. PMID: 23585445 English, Italian.
-
CDC National Health Report: leading causes of morbidity and mortality and associated behavioral risk and protective factors--United States, 2005-2013.MMWR Suppl. 2014 Oct 31;63(4):3-27. MMWR Suppl. 2014. PMID: 25356673
Cited by
-
Global patterns of mortality in international migrants: a systematic review and meta-analysis.Lancet. 2018 Dec 15;392(10164):2553-2566. doi: 10.1016/S0140-6736(18)32781-8. Epub 2018 Dec 5. Lancet. 2018. PMID: 30528484 Free PMC article.
-
Trends of under-five mortality and associated risk factors in Zambia: a multi survey analysis between 2007 and 2018.BMC Pediatr. 2022 Jun 13;22(1):341. doi: 10.1186/s12887-022-03362-7. BMC Pediatr. 2022. PMID: 35698091 Free PMC article.
References
-
- CDC Mortality among newly arrived Mozambican refugees, Zimbabwe and Malawai. MMWR. 1993;42(468–468):475–7. - PubMed
-
- Chaman R, Alami A, Emamian MH, Naieni KH, Mirmohammadkhani M, Ahmadnezhad E, Shariati M. Important risk factors of mortality among children aged 1–59months in rural areas of shahroud, Iran: A community based nested case-control study. Int J Prev Med. 2012;3(12):875–9. doi: 10.4103/2008-7802.104859. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
