

Medical Management of Glaucoma in the 21st Century from a Canadian Perspective
- PMID: 27895937
- PMCID: PMC5118538
- DOI: 10.1155/2016/6509809
Medical Management of Glaucoma in the 21st Century from a Canadian Perspective
Abstract
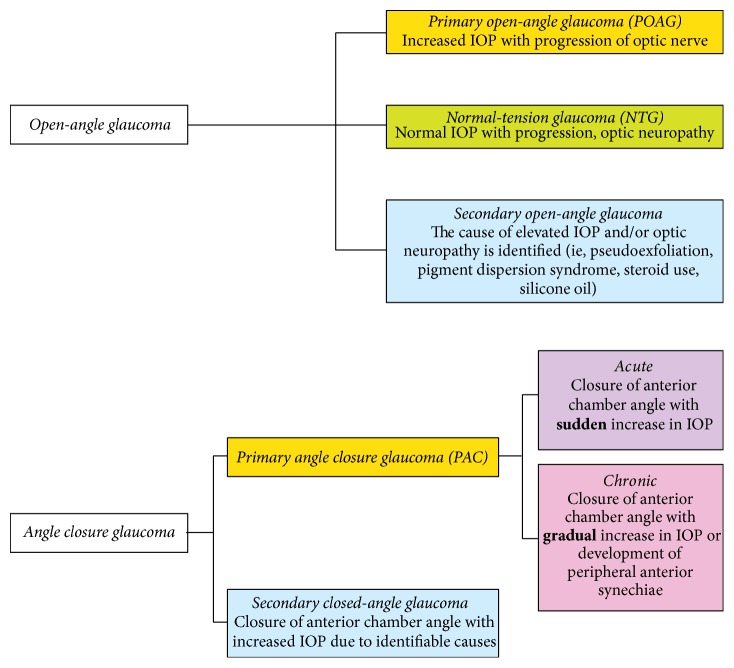
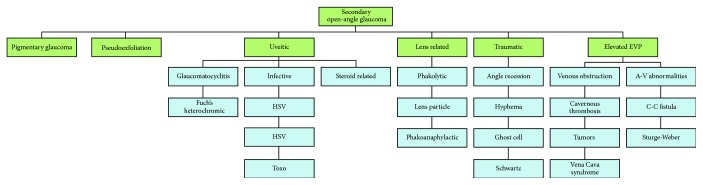
Glaucoma is a medical term describing a group of progressive optic neuropathies characterized by degeneration of retinal ganglion cells and retinal nerve fibre layer and resulting in changes in the optic nerve head. Glaucoma is a leading cause of irreversible vision loss worldwide. With the aging population it is expected that the prevalence of glaucoma will continue to increase. Despite recent advances in imaging and visual field testing techniques that allow establishment of earlier diagnosis and treatment initiation, significant numbers of glaucoma patients are undiagnosed and present late in the course of their disease. This can lead to irreversible vision loss, reduced quality of life, and a higher socioeconomic burden. Selection of therapeutic approaches for glaucoma should be based on careful ocular examination, patient medical history, presence of comorbidities, and awareness of concomitant systemic therapies. Therapy should also be individualized to patients' needs and preferences. Recent developments in this therapeutic field require revisiting treatment algorithms and integration of traditional and novel approaches in order to ensure optimal visual outcomes. This article provides an overview of recent developments and practice trends in the medical management of glaucoma in Canada. A discussion of the surgical management is beyond the scope of this paper.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- European Glaucoma Society. Terminology and Guidelines for Glaucoma. 4th. 2015. http://www.eugs.org/eng/EGS_guidelines4.asp. - PubMed
-
- Na J. H., Lee K., Lee J. R., Baek S., Yoo S. J., Kook M. S. Detection of macular ganglion cell loss in preperimetric glaucoma patients with localized retinal nerve fibre defects by spectral-domain optical coherence tomography. Clinical and Experimental Ophthalmology. 2013;41(9):870–880. doi: 10.1111/ceo.12142. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
