Uterine rupture in pregnancies following myomectomy: A multicenter case series
- PMID: 27896247
- PMCID: PMC5120064
- DOI: 10.5468/ogs.2016.59.6.454
Uterine rupture in pregnancies following myomectomy: A multicenter case series
Abstract
Objective: The purpose of this case series was to retrospectively examine records of cases with uterine rupture in pregnancies following myomectomy and to describe the clinical features and pregnancy outcomes.
Methods: This study was conducted as a multicenter case series. The patient databases at 7 tertiary hospitals were queried. Records of patients with a diagnosis of uterine rupture in the pregnancy following myomectomy between January 2012 and December 2014 were retrospectively collected. The uterine rupture cases enrolled in this study were defined as follows: through-and-through uterine rupture or tear of the uterine muscle and serosa, occurrence from 24+0 to 41+6 weeks' gestation, singleton pregnancy, and previous laparoscopic myomectomy (LSM) or laparotomic myomectomy (LTM) status.
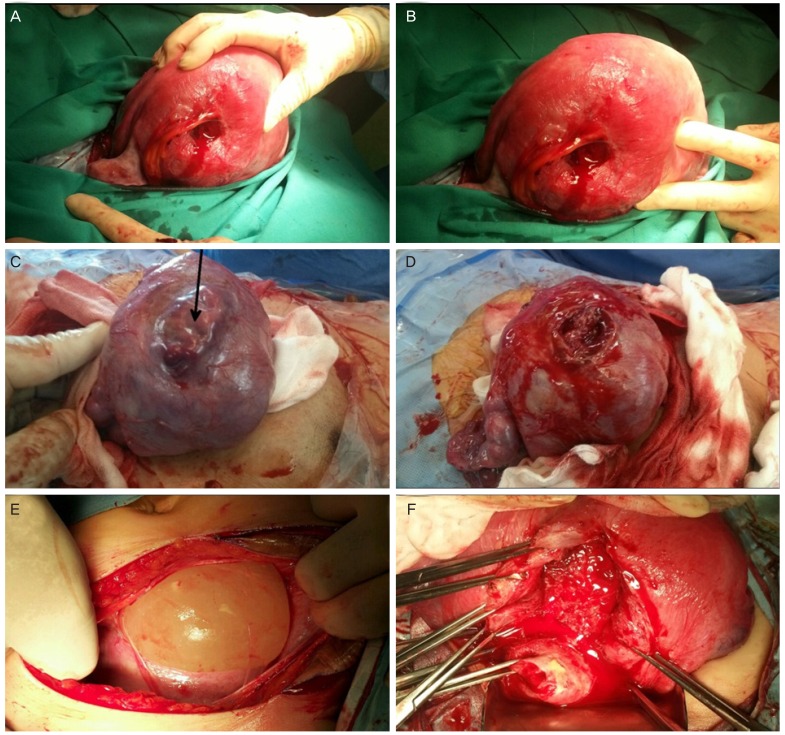
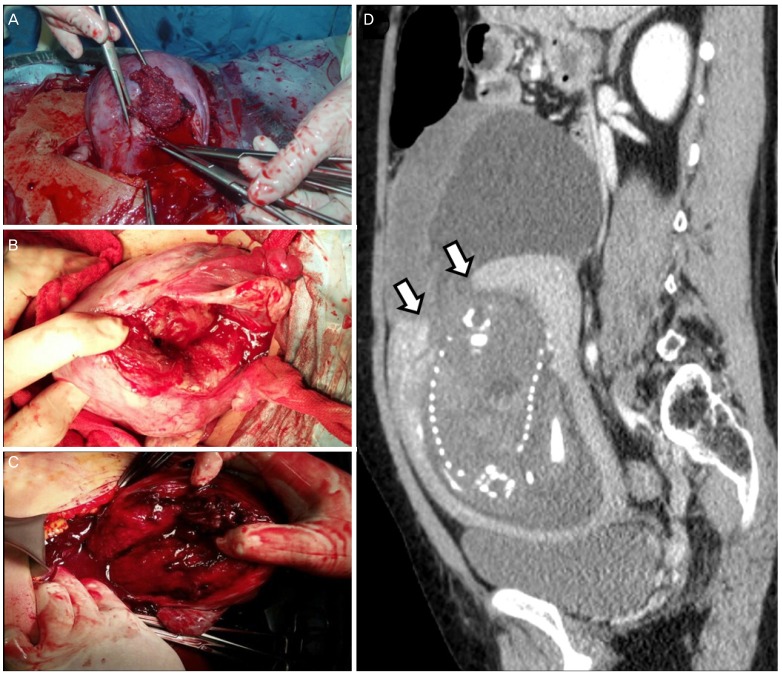
Results: Fourteen pregnant women experienced uterine rupture during their pregnancy after LSM or LTM. Preterm delivery of less than 34 weeks' gestation occurred in 5 cases, while intrauterine fetal death occurred in 3, and 3 cases had fetal distress. Of the 14 uterine rupture cases, none occurred during labor. All mothers survived and had no sequelae, unlike the perinatal outcomes, although they were receiving blood transfusion or treatment for uterine artery embolization because of uterine atony or massive hemorrhage.
Conclusion: In women of childbearing age who are scheduled to undergo LTM or LSM, the potential risk of uterine rupture on subsequent pregnancy should be explained before surgery. Pregnancy in women after myomectomy should be carefully observed, and they should be adequately counseled during this period.
Keywords: Myomectomy; Pregnancy outcome; Uterine rupture.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
Similar articles
-
Laparoscopic myomectomy and subsequent pregnancy: results in 54 patients.Hum Reprod. 2000 Sep;15(9):1993-6. doi: 10.1093/humrep/15.9.1993. Hum Reprod. 2000. PMID: 10967002
-
Pregnancy Outcomes and Risk Factors for Uterine Rupture After Laparoscopic Myomectomy: A Single-Center Experience and Literature Review.J Minim Invasive Gynecol. 2015 Sep-Oct;22(6):1022-8. doi: 10.1016/j.jmig.2015.05.016. Epub 2015 May 23. J Minim Invasive Gynecol. 2015. PMID: 26012718 Review.
-
Vaginal birth after prior myomectomy.Eur J Obstet Gynecol Reprod Biol. 2018 Dec;231:198-203. doi: 10.1016/j.ejogrb.2018.10.007. Epub 2018 Oct 3. Eur J Obstet Gynecol Reprod Biol. 2018. PMID: 30396109
-
Conservative management of uterine artery pseudoaneurysm after laparoscopic-assisted myomectomy and subsequent pregnancy outcome: case series and review of the literature.Eur J Obstet Gynecol Reprod Biol. 2014 Nov;182:146-53. doi: 10.1016/j.ejogrb.2014.09.020. Epub 2014 Sep 19. Eur J Obstet Gynecol Reprod Biol. 2014. PMID: 25277771 Review.
-
Obstetric outcomes after uterine myomectomy: Laparoscopic versus laparotomic approach.Obstet Gynecol Sci. 2013 Nov;56(6):375-81. doi: 10.5468/ogs.2013.56.6.375. Epub 2013 Nov 15. Obstet Gynecol Sci. 2013. PMID: 24396816 Free PMC article.
Cited by
-
Rupture of a myomectomy site in the third trimester of pregnancy after myomectomy, septoplasty and cesarean section: A case report.Case Rep Womens Health. 2018 May 30;19:e00066. doi: 10.1016/j.crwh.2018.e00066. eCollection 2018 Jul. Case Rep Womens Health. 2018. PMID: 30094194 Free PMC article.
-
Cystic Adenomyoma in Pregnancy: A Case Report.Int J Womens Health. 2024 Mar 7;16:421-432. doi: 10.2147/IJWH.S450701. eCollection 2024. Int J Womens Health. 2024. PMID: 38469356 Free PMC article.
-
Transvaginal radiofrequency ablation: a therapeutic option for managing symptomatic uterine fibroids in women with reproductive desires.F S Rep. 2024 Jul 15;5(3):320-327. doi: 10.1016/j.xfre.2024.07.001. eCollection 2024 Sep. F S Rep. 2024. PMID: 39381652 Free PMC article.
-
Unexpected early pregnancy during myomectomy followed by successful term delivery: A case report.Int J Reprod Biomed. 2024 Oct 14;22(8):673-678. doi: 10.18502/ijrm.v22i8.17242. eCollection 2024 Aug. Int J Reprod Biomed. 2024. PMID: 39494124 Free PMC article.
-
Risk Factors Associated with Uterine Rupture and Dehiscence: A Cross-Sectional Canadian Study.Rev Bras Ginecol Obstet. 2021 Nov;43(11):820-825. doi: 10.1055/s-0041-1739461. Epub 2021 Dec 6. Rev Bras Ginecol Obstet. 2021. PMID: 34872139 Free PMC article.
References
-
- Buttram VC, Jr, Reiter RC. Uterine leiomyomata: etiology, symptomatology, and management. Fertil Steril. 1981;36:433–445. - PubMed
-
- Carlson KJ, Miller BA, Fowler FJ., Jr The maine women’s health study: I. outcomes of hysterectomy. Obstet Gynecol. 1994;83:556–565. - PubMed
-
- Eldar-Geva T, Meagher S, Healy DL, MacLachlan V, Breheny S, Wood C. Effect of intramural, subserosal, and submucosal uterine fibroids on the outcome of assisted reproductive technology treatment. Fertil Steril. 1998;70:687–691. - PubMed
-
- Brady PC, Stanic AK, Styer AK. Uterine fibroids and subfertility: an update on the role of myomectomy. Curr Opin Obstet Gynecol. 2013;25:255–259. - PubMed
-
- Parazzini F, Tozzi L, Bianchi S. Pregnancy outcome and uterine fibroids. Best Pract Res Clin Obstet Gynaecol. 2016;34:74–84. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources