

Vitamin K antagonists: relative strengths and weaknesses vs. direct oral anticoagulants for stroke prevention in patients with atrial fibrillation
- PMID: 27896543
- PMCID: PMC5337242
- DOI: 10.1007/s11239-016-1446-0
Vitamin K antagonists: relative strengths and weaknesses vs. direct oral anticoagulants for stroke prevention in patients with atrial fibrillation
Abstract
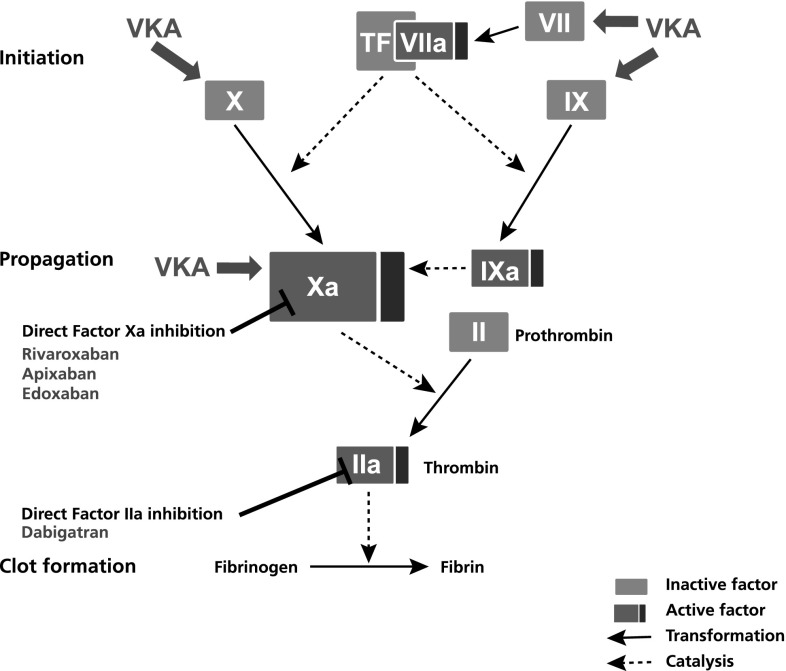
Vitamin K antagonists (VKAs) have been the mainstay of anticoagulation therapy for more than 50 years. VKAs are mainly used for the prevention of stroke in patients with atrial fibrillation (AF) and the treatment and secondary prevention of venous thromboembolism. In the past 5 years, four new agents-the direct factor Xa inhibitors apixaban, edoxaban and rivaroxaban and the direct thrombin inhibitor dabigatran [collectively known as direct oral anticoagulants (DOACs) or non-VKA oral anticoagulants]-have been approved for these and other indications. Despite these new treatment options, the VKA warfarin currently remains the most frequently prescribed oral anticoagulant. The availability of DOACs provides an alternative management option for patients with AF, especially when the treating physician is hesitant to prescribe a VKA owing to associated limitations, such as food and drug interactions, and concerns about bleeding complications. Currently available real-world evidence shows that DOACs have similar or improved effectiveness and safety outcomes compared with warfarin. Treatment decisions on which DOAC is best suited for which patient to maximize safety and effectiveness should take into account not only clinically relevant patient characteristics but also patient preference. This article reviews and highlights real and perceived implications of VKAs for the prevention of stroke in patients with non-valvular AF, with specific reference to their strengths and weaknesses compared with DOACs.
Keywords: Anticoagulants; Antithrombins; Atrial fibrillation; Factor Xa inhibitors; Stroke.
Conflict of interest statement
Conflict of interest
The authors declare no conflicts of interest in this work, and received no funding for it. Funding for editorial assistance was provided by Bayer AG.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Figures
References
-
- ACTIVE Writing Group of the ACTIVE Investigators Clopidogrel plus aspirin versus oral anticoagulation for atrial fibrillation in the atrial fibrillation clopidogrel trial with Irbesartan for prevention of vascular events (ACTIVE W): a randomised controlled trial. The Lancet. 2006;367:1903–1912. doi: 10.1016/S0140-6736(06)68845-4. - DOI - PubMed
-
- Ageno W, Gallus AS, Wittkowsky A, Crowther M, Hylek EM, Palareti G. Oral anticoagulant therapy: antithrombotic therapy and prevention of thrombosis, 9th ed: American college of chest physicians evidence-based clinical practice guidelines. Chest. 2012;141:e44S–e88S. doi: 10.1378/chest.11-2292. - DOI - PMC - PubMed
-
- Amin A, Bruno A, Trocio J, Lin J, Lingohr-Smith M. Comparison of differences in medical costs when new oral anticoagulants are used for the treatment of patients with non-valvular atrial fibrillation and venous thromboembolism vs. warfarin or placebo in the US. J Med Econ. 2015;18:399–409. doi: 10.3111/13696998.2015.1007210. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
