

Low skeletal muscle radiation attenuation and visceral adiposity are associated with overall survival and surgical site infections in patients with pancreatic cancer
- PMID: 27897432
- PMCID: PMC5377384
- DOI: 10.1002/jcsm.12155
Low skeletal muscle radiation attenuation and visceral adiposity are associated with overall survival and surgical site infections in patients with pancreatic cancer
Abstract
Background: Cancer cachexia and skeletal muscle wasting are related to poor survival. In this study, quantitative body composition measurements using computed tomography (CT) were investigated in relation to survival, post-operative complications, and surgical site infections in surgical patients with cancer of the head of the pancreas.
Methods: A prospective cohort of 199 patients with cancer of the head of the pancreas was analysed by CT imaging at the L3 level to determine (i) muscle radiation attenuation (average Hounsfield units of total L3 skeletal muscle); (ii) visceral adipose tissue area; (iii) subcutaneous adipose tissue area; (iv) intermuscular adipose tissue area; and (v) skeletal muscle area. Sex-specific cut-offs were determined at the lower tertile for muscle radiation attenuation and skeletal muscle area and the higher tertile for adipose tissues. These variables of body composition were related to overall survival, severe post-operative complications (Dindo-Clavien ≥ 3), and surgical site infections (wounds inspected daily by an independent trial nurse) using Cox-regression analysis and multivariable logistic regression analysis, respectively.
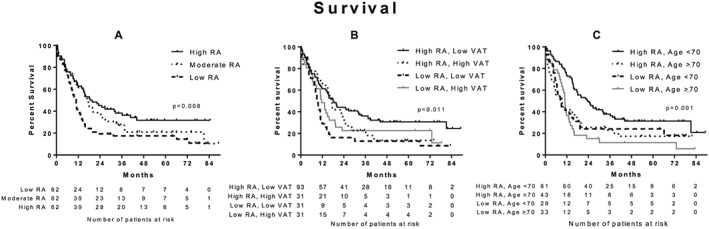
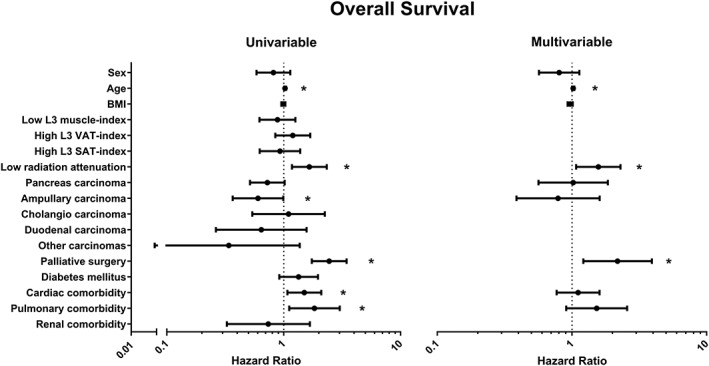
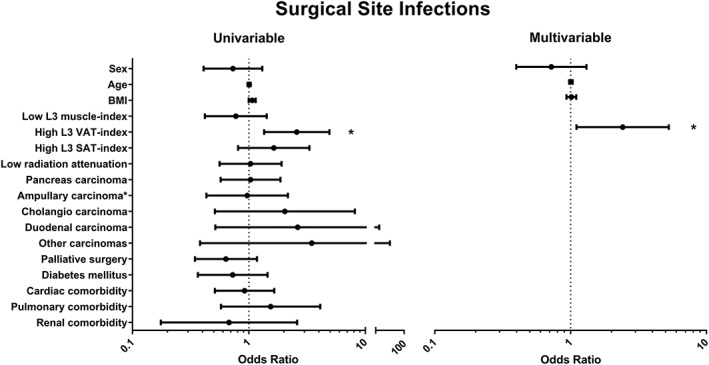
Results: Low muscle radiation attenuation was associated with shorter survival in comparison with moderate and high muscle radiation attenuation [median survival 10.8 (95% CI: 8.8-12.8) vs. 17.4 (95% CI: 14.7-20.1), and 18.5 (95% CI: 9.2-27.8) months, respectively; P < 0.008]. Patient subgroups with high muscle radiation attenuation combined with either low visceral adipose tissue or age <70 years had longer survival than other subgroups (P = 0.011 and P = 0.001, respectively). Muscle radiation attenuation was inversely correlated with intermuscular adipose tissue (rp = -0.697, P < 0.001). High visceral adipose tissue was associated with an increased surgical site infection rate, OR: 2.4 (95% CI: 1.1-5.3; P = 0.027).
Conclusions: Low muscle radiation attenuation was associated with reduced survival, and high visceral adiposity was associated with an increase in surgical site infections. The strong correlation between muscle radiation attenuation and intermuscular adipose tissue suggests the presence of ectopic fat in muscle, warranting further investigation. CT image analysis could be implemented in pre-operative risk assessment to assist in treatment decision-making.
Keywords: Body composition; Computed tomography; Pancreatic cancer; Radiation attenuation; Surgical site infection; Visceral adipose tissue.
© 2016 The Authors. Journal of Cachexia, Sarcopenia and Muscle published by John Wiley & Sons Ltd on behalf of the Society on Sarcopenia, Cachexia and Wasting Disorders.
Figures
References
-
- Nederlandse Kankerregistratie [database on the Internet] 1989. Available from: http://cijfersoverkanker.nl/. Accessed: February 1, 2012
-
- Fearon K, Strasser F, Anker SD, Bosaeus I, Bruera E, Fainsinger RL, et al. Definition and classification of cancer cachexia: an international consensus. Lancet Oncol 2011;12:489–95. - PubMed
-
- Dewys W, Begg C, Lavin P, Band P, Bennett J, Bertino J, et al. Prognostic effect of weight loss prior to chemotherapy in cancer patients. Eastern Cooperative Oncology Group. Am J Med 1980;69:491–7. - PubMed
-
- van der Gaag NA, Harmsen K, Eshuis WJ, Busch OR, van Gulik TM, Gouma DJ. Pancreatoduodenectomy associated complications influence cancer recurrence and time interval to death. Eur J Surg Oncol 2014;40:551–8. - PubMed
-
- Sugiura T, Uesaka K, Ohmagari N, Kanemoto H, Mizuno T. Risk factor of surgical site infection after pancreaticoduodenectomy. World J Surg 2012;36:2888–94. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
