

Limiting sedation for patients with acute respiratory distress syndrome - time to wake up
- PMID: 27898439
- PMCID: PMC5729753
- DOI: 10.1097/MCC.0000000000000382
Limiting sedation for patients with acute respiratory distress syndrome - time to wake up
Abstract
Purpose of review: Critically ill patients with acute respiratory distress syndrome (ARDS) may require sedation in their clinical care. The goals of sedation in ARDS patients are to improve patient comfort and tolerance of supportive and therapeutic measures without contributing to adverse outcomes. This review discusses the current evidence for sedation management in patients with ARDS.
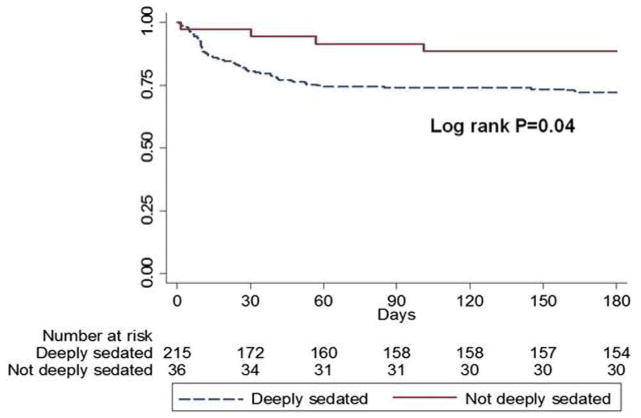
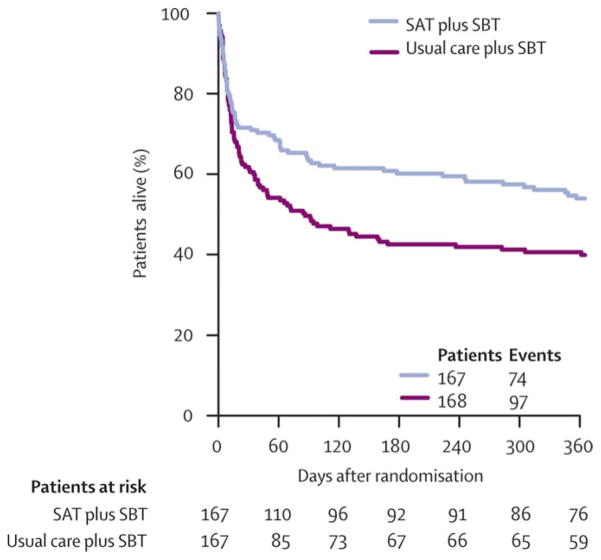
Recent findings: Deep sedation strategies should be avoided in the care of patients with ARDS because deep sedation has been associated with increased time on mechanical ventilation, longer ICU and hospital length of stay, and higher mortality in critically ill patients. Adoption of protocol-based, light-sedation strategies is preferred and improves patient outcomes. Although the optimal sedative agent for ARDS patients is unclear, benzodiazepines should be avoided because of associations with oversedation, delirium, prolonged ICU and hospital length of stay, and increased mortality. Minimizing sedation in patients with ARDS facilitates early mobilization and early discharge from the ICU, potentially aiding in recovery from critical illness. Strategies to optimize ventilation in ARDS patients, such as low tidal volume ventilation and high positive end-expiratory pressure can be employed without deep sedation; however, deep sedation is required if patients receive neuromuscular blockade, which may benefit some ARDS patients. Knowledge gaps persist as to whether or not prone positioning and extracorporeal membrane oxygenation can be tolerated with light sedation.
Summary: Current evidence supports the use of protocol-based, light-sedation strategies in critically ill patients with ARDS. Further research into sedation management specifically in ARDS populations is needed.
Figures
References
-
- Kress JP, Pohlman AS, O’Connor MF, Hall JB. Daily interruption of sedative infusions in critically ill patients undergoing mechanical ventilation. The New England journal of medicine. 2000 May 18;342(20):1471–1477. - PubMed
-
- Pandharipande PP, Pun BT, Herr DL, et al. Effect of sedation with dexmedetomidine vs lorazepam on acute brain dysfunction in mechanically ventilated patients: the MENDS randomized controlled trial. Jama. 2007 Dec 12;298(22):2644–2653. - PubMed
-
- Girard TD, Kress JP, Fuchs BD, et al. Efficacy and safety of a paired sedation and ventilator weaning protocol for mechanically ventilated patients in intensive care (Awakening and Breathing Controlled trial): a randomised controlled trial. Lancet. 2008 Jan 12;371(9607):126–134. - PubMed
-
- Mehta S, Burry L, Cook D, et al. Daily sedation interruption in mechanically ventilated critically ill patients cared for with a sedation protocol: a randomized controlled trial. Jama. 2012 Nov 21;308(19):1985–1992. - PubMed
-
- Weinert CR, Calvin AD. Epidemiology of sedation and sedation adequacy for mechanically ventilated patients in a medical and surgical intensive care unit. Critical care medicine. 2007 Feb;35(2):393–401. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
