

Patient-Reported Barriers to Adherence to Antiretroviral Therapy: A Systematic Review and Meta-Analysis
- PMID: 27898679
- PMCID: PMC5127502
- DOI: 10.1371/journal.pmed.1002183
Patient-Reported Barriers to Adherence to Antiretroviral Therapy: A Systematic Review and Meta-Analysis
Abstract
Background: Maintaining high levels of adherence to antiretroviral therapy (ART) is a challenge across settings and populations. Understanding the relative importance of different barriers to adherence will help inform the targeting of different interventions and future research priorities.
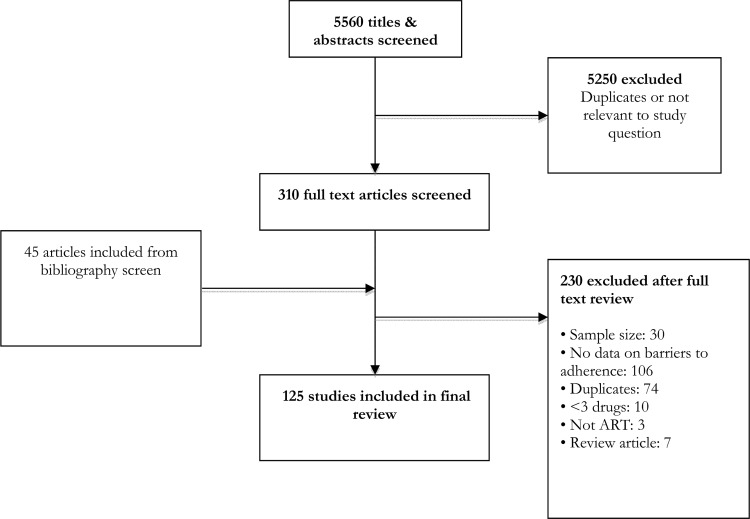
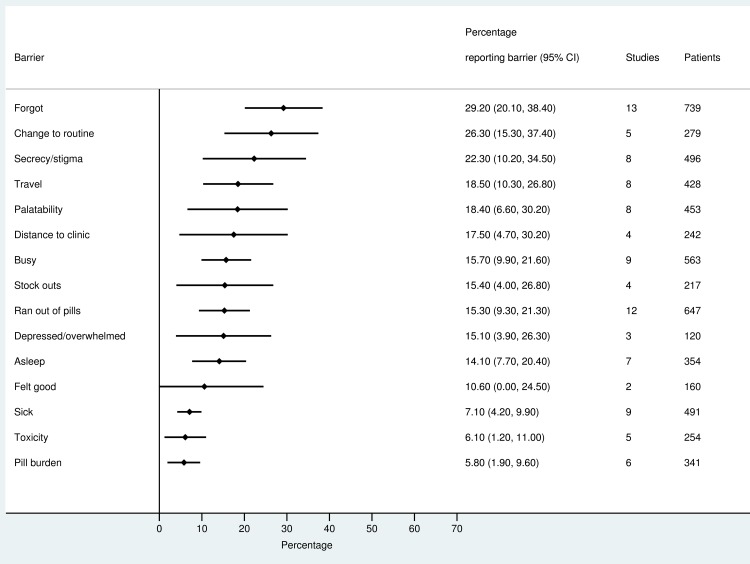
Methods and findings: We searched MEDLINE via PubMed, Embase, Web of Science, and PsychINFO from 01 January 1997 to 31 March 2016 for studies reporting barriers to adherence to ART. We calculated pooled proportions of reported barriers to adherence per age group (adults, adolescents, and children). We included data from 125 studies that provided information about adherence barriers for 17,061 adults, 1,099 children, and 856 adolescents. We assessed differences according to geographical location and level of economic development. The most frequently reported individual barriers included forgetting (adults 41.4%, 95% CI 37.3%-45.4%; adolescents 63.1%, 95% CI 46.3%-80.0%; children/caregivers 29.2%, 95% CI 20.1%-38.4%), being away from home (adults 30.4%, 95% CI 25.5%-35.2%; adolescents 40.7%, 95% CI 25.7%-55.6%; children/caregivers 18.5%, 95% CI 10.3%-26.8%), and a change to daily routine (adults 28.0%, 95% CI 20.9%-35.0%; adolescents 32.4%, 95% CI 0%-75.0%; children/caregivers 26.3%, 95% CI 15.3%-37.4%). Depression was reported as a barrier to adherence by more than 15% of patients across all age categories (adults 15.5%, 95% CI 12.8%-18.3%; adolescents 25.7%, 95% CI 17.7%-33.6%; children 15.1%, 95% CI 3.9%-26.3%), while alcohol/substance misuse was commonly reported by adults (12.9%, 95% CI 9.7%-16.1%) and adolescents (28.8%, 95% CI 11.8%-45.8%). Secrecy/stigma was a commonly cited barrier to adherence, reported by more than 10% of adults and children across all regions (adults 13.6%, 95% CI 11.9%-15.3%; children/caregivers 22.3%, 95% CI 10.2%-34.5%). Among adults, feeling sick (15.9%, 95% CI 13.0%-18.8%) was a more commonly cited barrier to adherence than feeling well (9.3%, 95% CI 7.2%-11.4%). Health service-related barriers, including distance to clinic (adults 17.5%, 95% CI 13.0%-21.9%) and stock outs (adults 16.1%, 95% CI 11.7%-20.4%), were also frequently reported. Limitations of this review relate to the fact that included studies differed in approaches to assessing adherence barriers and included variable durations of follow up. Studies that report self-reported adherence will likely underestimate the frequency of non-adherence. For children, barriers were mainly reported by caregivers, which may not correspond to the most important barriers faced by children.
Conclusions: Patients on ART face multiple barriers to adherence, and no single intervention will be sufficient to ensure that high levels of adherence to treatment and virological suppression are sustained. For maximum efficacy, health providers should consider a more triaged approach that first identifies patients at risk of poor adherence and then seeks to establish the support that is needed to overcome the most important barriers to adherence.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures


References
-
- Bangsberg DR, Perry S, Charlebois ED, Clark RA, Roberston M, Zolopa AR, et al. Non-adherence to highly active antiretroviral therapy predicts progression to AIDS. AIDS. 2001;15(9):1181–3. . - PubMed
-
- Martin M, Del Cacho E, Codina C, Tuset M, De Lazzari E, Mallolas J, et al. Relationship between adherence level, type of the antiretroviral regimen, and plasma HIV type 1 RNA viral load: a prospective cohort study. AIDS Res Hum Retroviruses. 2008;24(10):1263–8. 10.1089/aid.2008.0141 . - DOI - PubMed
-
- Nachega JB, Hislop M, Dowdy DW, Lo M, Omer SB, Regensberg L, et al. Adherence to highly active antiretroviral therapy assessed by pharmacy claims predicts survival in HIV-infected South African adults. J Acquir Immune Defic Syndr. 2006;43(1):78–84. 10.1097/01.qai.0000225015.43266.46 . - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
