

Relationships between Mucosal Antibodies, Non-Typeable Haemophilus influenzae (NTHi) Infection and Airway Inflammation in COPD
- PMID: 27898728
- PMCID: PMC5127575
- DOI: 10.1371/journal.pone.0167250
Relationships between Mucosal Antibodies, Non-Typeable Haemophilus influenzae (NTHi) Infection and Airway Inflammation in COPD
Erratum in
-
Correction: Relationships between Mucosal Antibodies, Non-Typeable Haemophilus influenzae (NTHi) Infection and Airway Inflammation in COPD.PLoS One. 2017 Apr 25;12(4):e0176749. doi: 10.1371/journal.pone.0176749. eCollection 2017. PLoS One. 2017. PMID: 28441440 Free PMC article.
Abstract
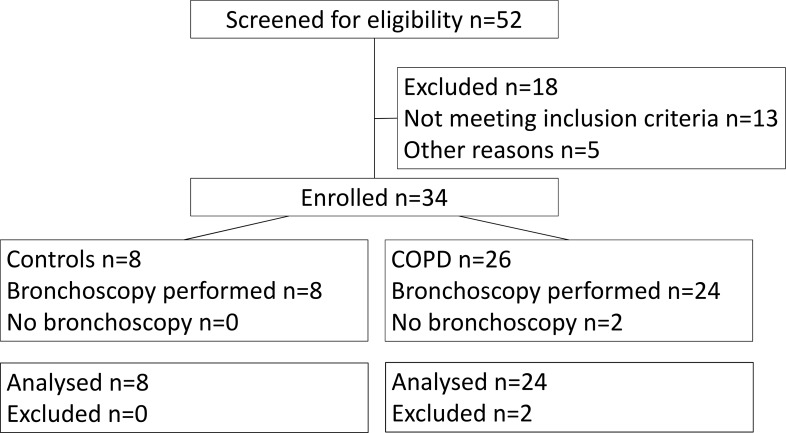
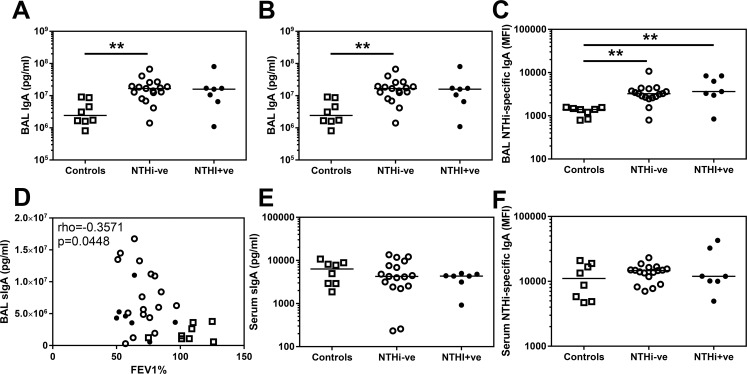
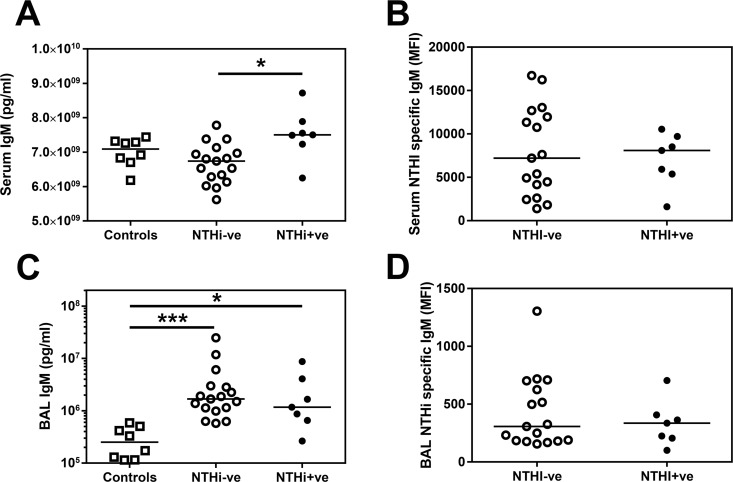
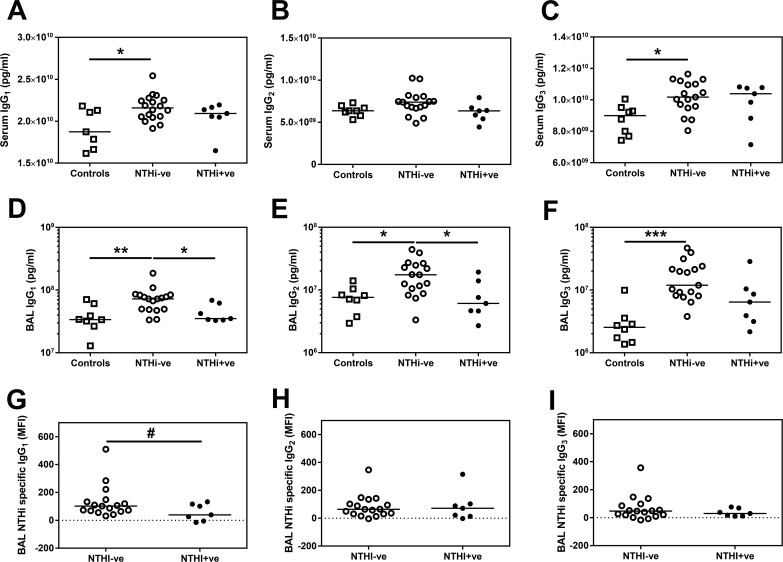
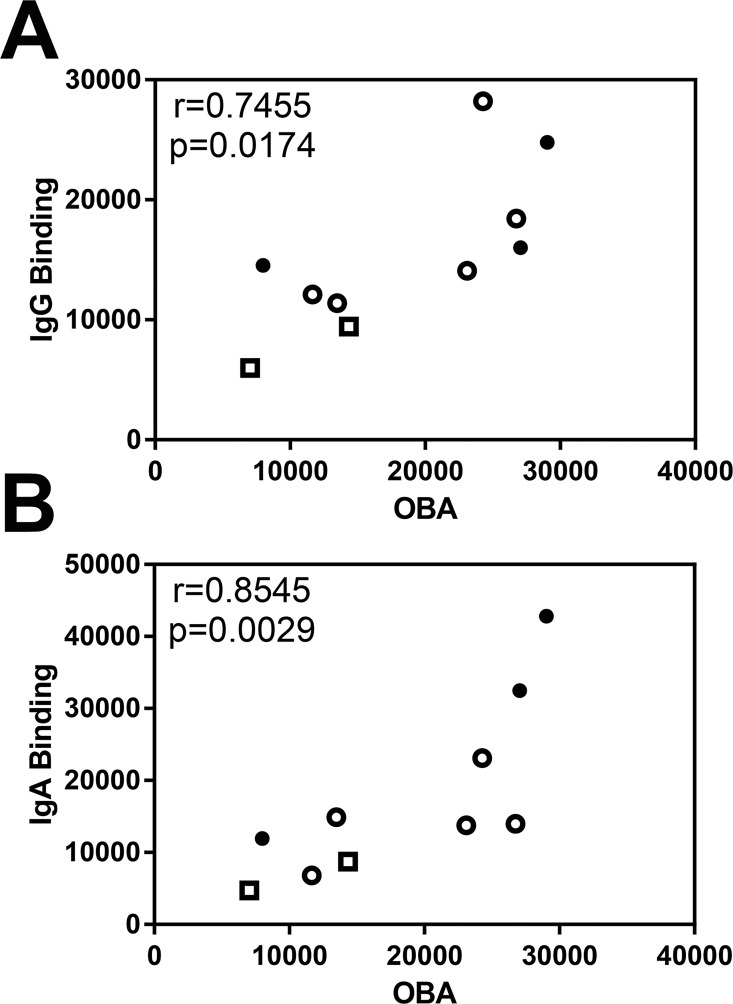
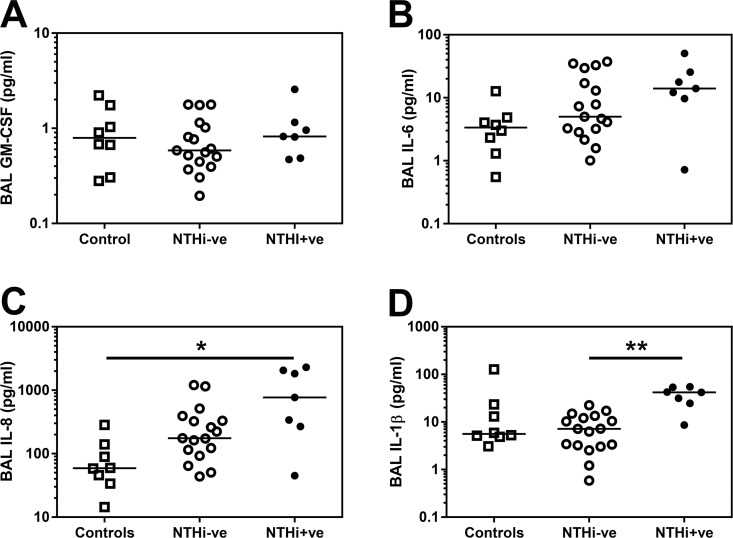
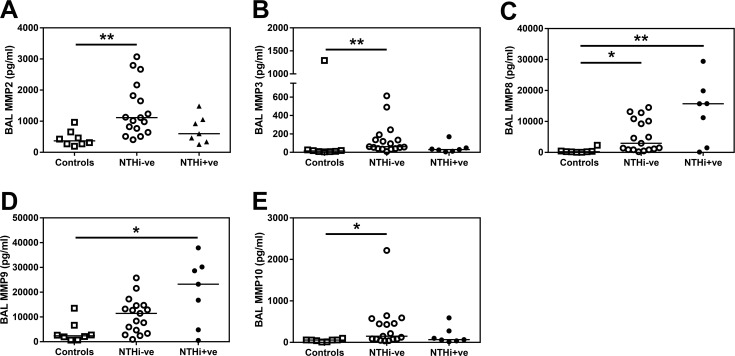
Non-typeable Haemophilus influenzae (NTHi) is a key pathogen in COPD, being associated with airway inflammation and risk of exacerbation. Why some patients are susceptible to colonisation is not understood. We hypothesised that this susceptibility may be due to a deficiency in mucosal humoral immunity. The aim of our study (NCT01701869) was to quantify the amount and specificity of antibodies against NTHi in the lungs and the associated risk of infection and inflammation in health and COPD. Phlebotomy, sputum induction and bronchoscopy were performed on 24 mild-to-moderate COPD patients and 8 age and smoking-matched controls. BAL (Bronchoalveolar lavage) total IgG1, IgG2, IgG3, IgM and IgA concentrations were significantly increased in COPD patients compared to controls. NTHi was detected in the lungs of 7 of the COPD patients (NTHi+ve-29%) and these patients had a higher median number of previous exacerbations than NTHi-ve patients as well as evidence of increased systemic inflammation. When comparing NTHi+ve versus NTHi-ve patients we observed a decrease in the amount of both total IgG1 (p = 0.0068) and NTHi-specific IgG1 (p = 0.0433) in the BAL of NTHi+ve patients, but no differences in total IgA or IgM. We observed no evidence of decreased IgG1 in the serum of NTHi+ve patients, suggesting this phenomenon is restricted to the airway. Furthermore, the NTHi+ve patients had significantly greater levels of IL-1β (p = 0.0003), in BAL than NTHi-ve COPD patients.This study indicates that the presence of NTHi is associated with reduced levels and function of IgG1 in the airway of NTHi-colonised COPD patients. This decrease in total and NTHI-specific IgG1 was associated with greater systemic and airway inflammation and a history of more frequent exacerbations and may explain the susceptibility of some COPD patients to the impacts of NTHi.
Conflict of interest statement
TGP is an employee of the GSK group of companies; he owns shares in GSK. These interests do not alter our adherence to PLOS ONE policies on sharing data and materials. The remaining authors have declared that no competing interests exist.
Figures
References
-
- Singh R, Mackay AJ, Patel AR, Garcha DS, Kowlessar BS, Brill SE, et al. Inflammatory thresholds and the species-specific effects of colonising bacteria in stable chronic obstructive pulmonary disease. Respir Res. 2014;15:114 PubMed Central PMCID: PMCPMC4173051. 10.1186/s12931-014-0114-1 - DOI - PMC - PubMed
-
- Bafadhel M, Haldar K, Barker B, Patel H, Mistry V, Barer MR, et al. Airway bacteria measured by quantitative polymerase chain reaction and culture in patients with stable COPD: relationship with neutrophilic airway inflammation, exacerbation frequency, and lung function. Int J Chron Obstruct Pulmon Dis. 2015;10:1075–83. PubMed Central PMCID: PMCPMC4468933. 10.2147/COPD.S80091 - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
