

Clinical determinants of the severity of Middle East respiratory syndrome (MERS): a systematic review and meta-analysis
- PMID: 27899100
- PMCID: PMC5129628
- DOI: 10.1186/s12889-016-3881-4
Clinical determinants of the severity of Middle East respiratory syndrome (MERS): a systematic review and meta-analysis
Abstract
Background: While the risk of severe complications of Middle East respiratory syndrome (MERS) and its determinants have been explored in previous studies, a systematic analysis of published articles with different designs and populations has yet to be conducted. The present study aimed to systematically review the risk of death associated with MERS as well as risk factors for associated complications.
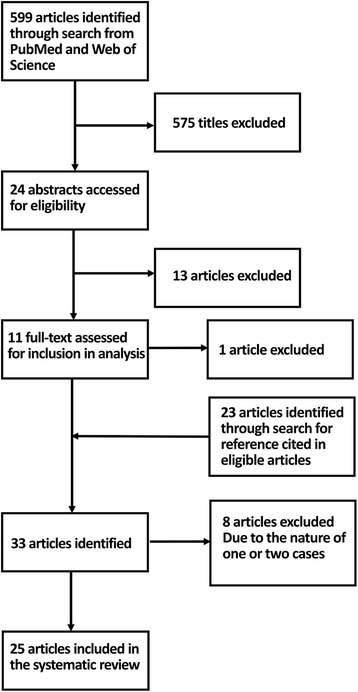
Methods: PubMed and Web of Science databases were searched for clinical and epidemiological studies on confirmed cases of MERS. Eligible articles reported clinical outcomes, especially severe complications or death associated with MERS. Risks of admission to intensive care unit (ICU), mechanical ventilation and death were estimated. Subsequently, potential associations between MERS-associated death and age, sex, underlying medical conditions and study design were explored.
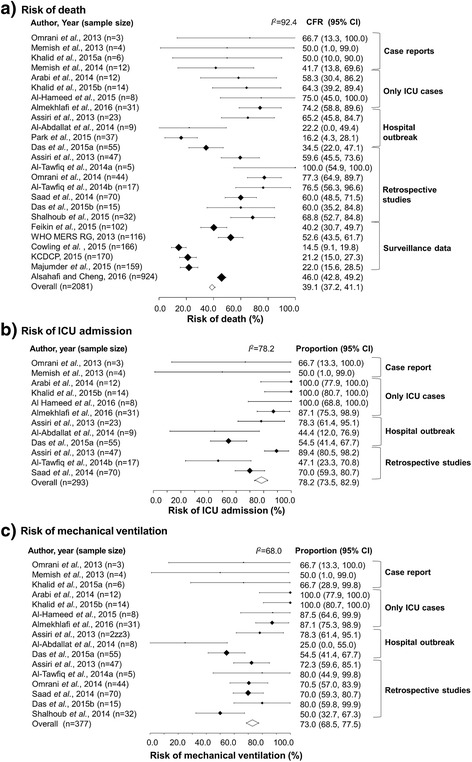
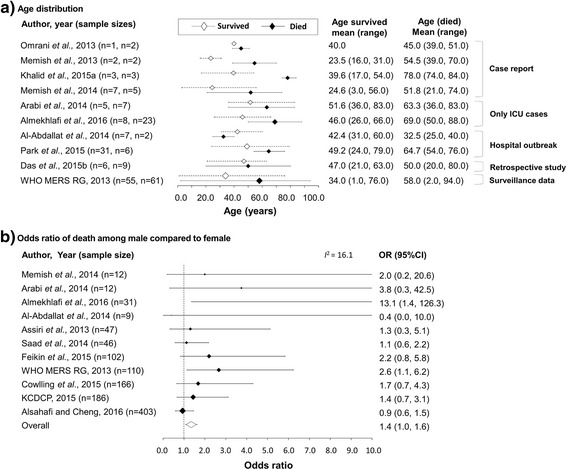
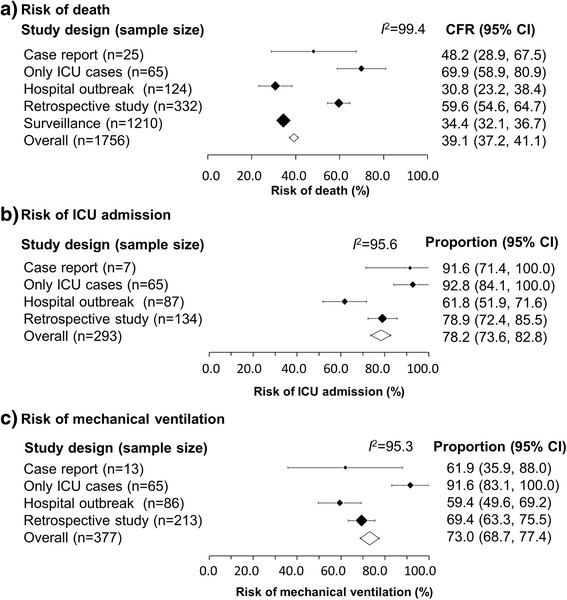
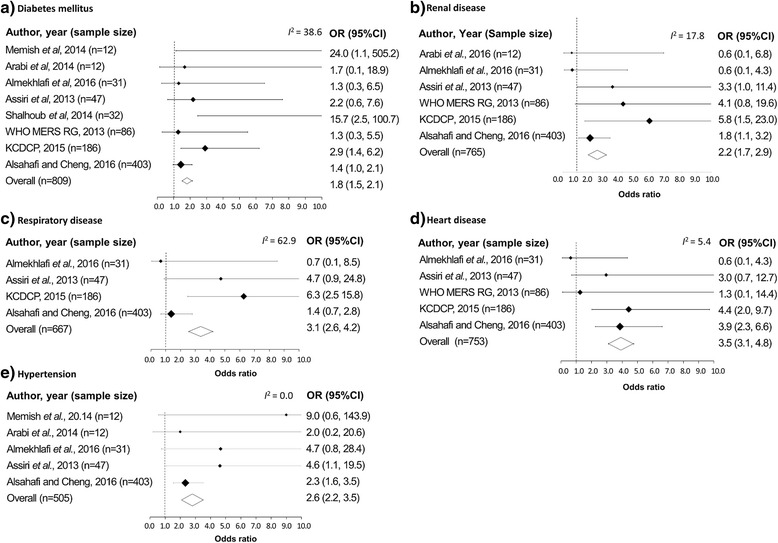
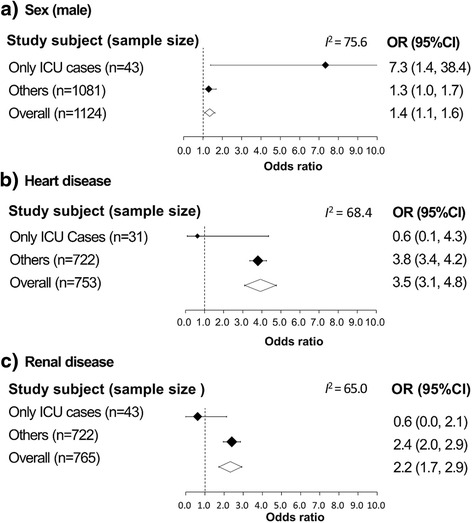
Results: A total of 25 eligible articles were identified. The case fatality risk ranged from 14.5 to 100%, with the pooled estimate at 39.1%. The risks of ICU admission and mechanical ventilation ranged from 44.4 to 100% and from 25.0 to 100%, with pooled estimates at 78.2 and 73.0%, respectively. These risks showed a substantial heterogeneity among the identified studies, and appeared to be the highest in case studies focusing on ICU cases. We identified older age, male sex and underlying medical conditions, including diabetes mellitus, renal disease, respiratory disease, heart disease and hypertension, as clinical predictors of death associated with MERS. In ICU case studies, the expected odds ratios (OR) of death among patients with underlying heart disease or renal disease to patients without such comorbidities were 0.6 (95% Confidence Interval (CI): 0.1, 4.3) and 0.6 (95% CI: 0.0, 2.1), respectively, while the ORs were 3.8 (95% CI: 3.4, 4.2) and 2.4 (95% CI: 2.0, 2.9), respectively, in studies with other types of designs.
Conclusions: The heterogeneity for the risk of death and severe manifestations was substantially high among the studies, and varying study designs was one of the underlying reasons for this heterogeneity. A statistical estimation of the risk of MERS death and identification of risk factors must be conducted, particularly considering the study design and potential biases associated with case detection and diagnosis.
Keywords: Ascertainment bias; Case fatality ratio; Comorbidity; Middle East respiratory syndrome.
Figures
Similar articles
-
Intravenous magnesium sulphate and sotalol for prevention of atrial fibrillation after coronary artery bypass surgery: a systematic review and economic evaluation.Health Technol Assess. 2008 Jun;12(28):iii-iv, ix-95. doi: 10.3310/hta12280. Health Technol Assess. 2008. PMID: 18547499
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
-
Behavioral interventions to reduce risk for sexual transmission of HIV among men who have sex with men.Cochrane Database Syst Rev. 2008 Jul 16;(3):CD001230. doi: 10.1002/14651858.CD001230.pub2. Cochrane Database Syst Rev. 2008. PMID: 18646068
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
-
Prognosis of adults and children following a first unprovoked seizure.Cochrane Database Syst Rev. 2023 Jan 23;1(1):CD013847. doi: 10.1002/14651858.CD013847.pub2. Cochrane Database Syst Rev. 2023. PMID: 36688481 Free PMC article.
Cited by
-
Retrospective Analysis of the Effect of Postmenopausal Women Medications on SARS-CoV-2 Infection Progression.Life (Basel). 2024 Sep 3;14(9):1107. doi: 10.3390/life14091107. Life (Basel). 2024. PMID: 39337891 Free PMC article.
-
The burden and risks of emerging complications of diabetes mellitus.Nat Rev Endocrinol. 2022 Sep;18(9):525-539. doi: 10.1038/s41574-022-00690-7. Epub 2022 Jun 6. Nat Rev Endocrinol. 2022. PMID: 35668219 Free PMC article. Review.
-
Comorbidity and its impact on 1590 patients with COVID-19 in China: a nationwide analysis.Eur Respir J. 2020 May 14;55(5):2000547. doi: 10.1183/13993003.00547-2020. Print 2020 May. Eur Respir J. 2020. PMID: 32217650 Free PMC article.
-
Meta-analysis and comprehensive study of coronavirus outbreaks: SARS, MERS and COVID-19.J Infect Public Health. 2021 Aug;14(8):1051-1064. doi: 10.1016/j.jiph.2021.06.007. Epub 2021 Jun 17. J Infect Public Health. 2021. PMID: 34174535 Free PMC article.
-
Exploration of sex-specific and age-dependent COVID-19 fatality rate in Bangladesh population.World J Radiol. 2021 Jan 28;13(1):1-18. doi: 10.4329/wjr.v13.i1.1. World J Radiol. 2021. PMID: 33574990 Free PMC article. Review.
References
-
- World Health Organization . Middle East respiratory syndrome coronavirus (MERS-CoV) Geneva: World Health Organization; 2016.
-
- Pebody RG, Chand MA, Thomas HL, Green HK, Boddington NL, Carvalho C, et al. The United Kingdom public health response to an imported laboratory confirmed case of a novel coronavirus in September 2012. Euro Surveill. 2012;17:20292. - PubMed
-
- Mailles A, Blanckaert K, Chaud P, van der Werf S, Lina B, Caro V, et al. First cases of middle east respiratory syndrome coronavirus (MERS-COV) infections in France, investigations and implications for the prevention of human-to-human transmission, France, May 2013. Euro Surveill. 2013;18:20502. - PubMed
-
- Kelly H, Cowling BJ. Case fatality: rate, ratio, or risk? Euro Surveill. 2013;24:622–3. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
