

Cardiac T1 Mapping and Extracellular Volume (ECV) in clinical practice: a comprehensive review
- PMID: 27899132
- PMCID: PMC5129251
- DOI: 10.1186/s12968-016-0308-4
Cardiac T1 Mapping and Extracellular Volume (ECV) in clinical practice: a comprehensive review
Abstract
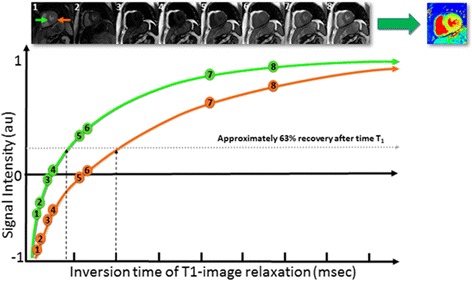
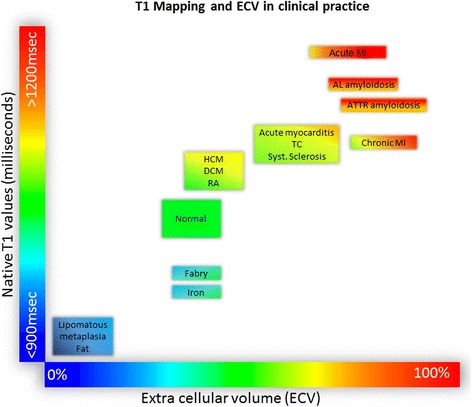
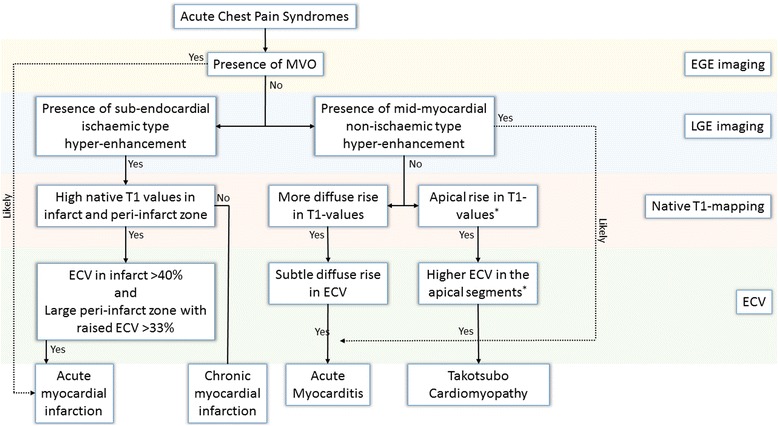
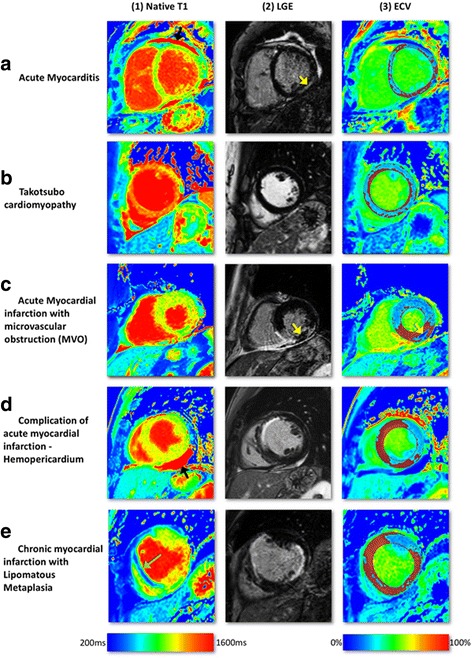
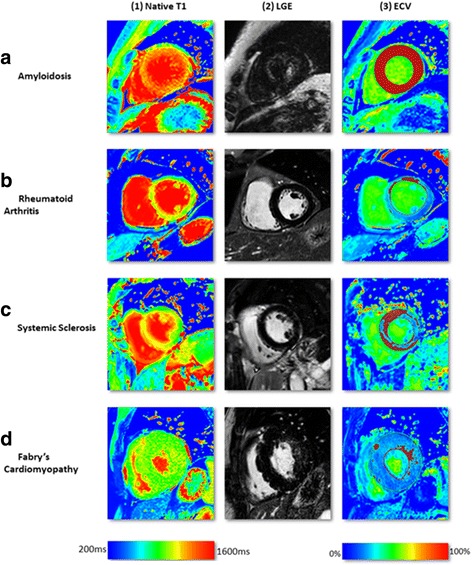
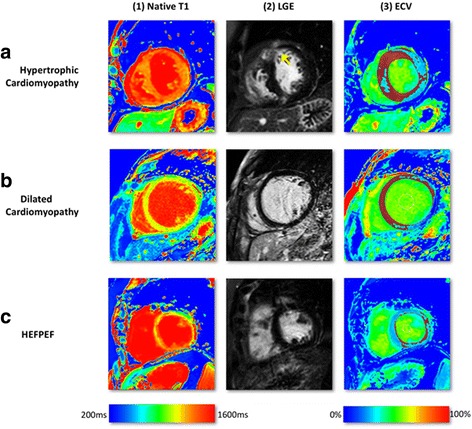
Cardiovascular Magnetic Resonance is increasingly used to differentiate the aetiology of cardiomyopathies. Late Gadolinium Enhancement (LGE) is the reference standard for non-invasive imaging of myocardial scar and focal fibrosis and is valuable in the differential diagnosis of ischaemic versus non-ischaemic cardiomyopathy. Diffuse fibrosis may go undetected on LGE imaging. Tissue characterisation with parametric mapping methods has the potential to detect and quantify both focal and diffuse alterations in myocardial structure not assessable by LGE. Native and post-contrast T1 mapping in particular has shown promise as a novel biomarker to support diagnostic, therapeutic and prognostic decision making in ischaemic and non-ischaemic cardiomyopathies as well as in patients with acute chest pain syndromes. Furthermore, changes in the myocardium over time may be assessed longitudinally with this non-invasive tissue characterisation method.
Keywords: Acute chest pain syndromes; Cardiomyopathy; Diffuse myocardial fibrosis; ECV; T1 mapping.
Figures
References
-
- Hundley WG, Bluemke DA, Finn JP, Flamm SD, Fogel MA, Friedrich MG, Ho VB, Jerosch-Herold M, Kramer CM, Manning WJ, Patel M, Pohost GM, Stillman AE, White RD, Woodard PK. ACCF/ACR/AHA/NASCI/SCMR 2010 expert consensus document on cardiovascular magnetic resonance: a report of the american college of cardiology foundation task force on expert consensus documents. J Am Coll Cardiol. 2010;55:2614–62. doi: 10.1016/j.jacc.2009.11.011. - DOI - PMC - PubMed
-
- Gulati A, Jabbour A, Ismail TF, Guha K, Khwaja J, Raza S, Morarji K, Brown TD, Ismail NA, Dweck MR, Di Pietro E, Roughton M, Wage R, Daryani Y, O’Hanlon R, Sheppard MN, Alpendurada F, Lyon AR, Cook SA, Cowie MR, Assomull RG, Pennell DJ, Prasad SK. Association of fibrosis with mortality and sudden cardiac death in patients with nonischemic dilated cardiomyopathy. JAMA. 2013;309:896–908. doi: 10.1001/jama.2013.1363. - DOI - PubMed
-
- Look DC, Locker DR. Time saving in measurement of NMR and EPR relaxation times. Rev Sci Instrum. 1970;41:250–1. doi: 10.1063/1.1684482. - DOI
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
