

Comparison between standard and reduced volume radiotherapy in bladder preservation trimodality protocol for muscle-invasive bladder cancer patients
- PMID: 27899955
- PMCID: PMC5102689
- DOI: 10.3332/ecancer.2016.682
Comparison between standard and reduced volume radiotherapy in bladder preservation trimodality protocol for muscle-invasive bladder cancer patients
Abstract
Aim: Our aim is to compare the toxicity, pelvic nodal relapse, and overall survival of whole bladder irradiation only to the standard technique of whole pelvis irradiation followed by bladder boost in patients with muscle-invasive bladder carcinoma undergoing bladder preservation protocol.
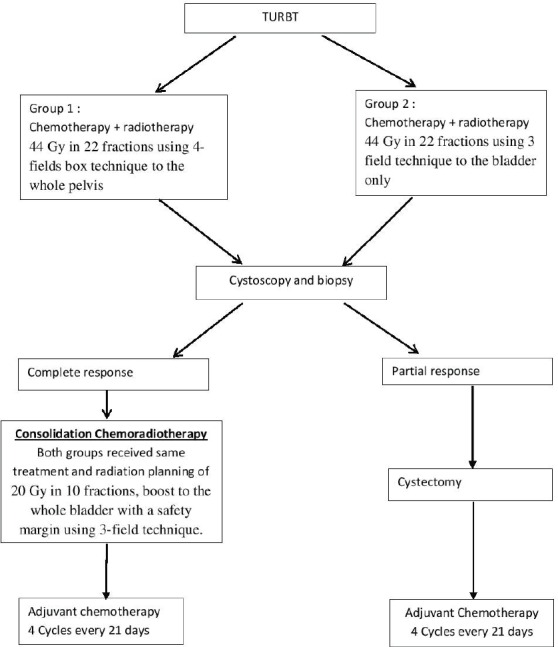
Material and method: A total of 60 patients with transitional cell carcinoma, stage T2-3, N0, M0 bladder cancer were subjected to maximal transurethral resection bladder tumour (TURB). Then, the patients were randomised into two groups: group I (30 patients) to receive whole pelvis radiotherapy 44 Gy followed by 20 Gy bladder boost. While group II (30 patients) were randomised to receive whole bladder radiotherapy alone for a total dose of 64 Gy. In both groups, concomitant cisplatin and paclitaxel were given weekly throughout the whole course of radiotherapy where conventional 2 Gy/fraction were used. Additionally, four cycles of adjuvant cisplatin and paclitaxel were given after the end of the chemoradiotherapy induction course.
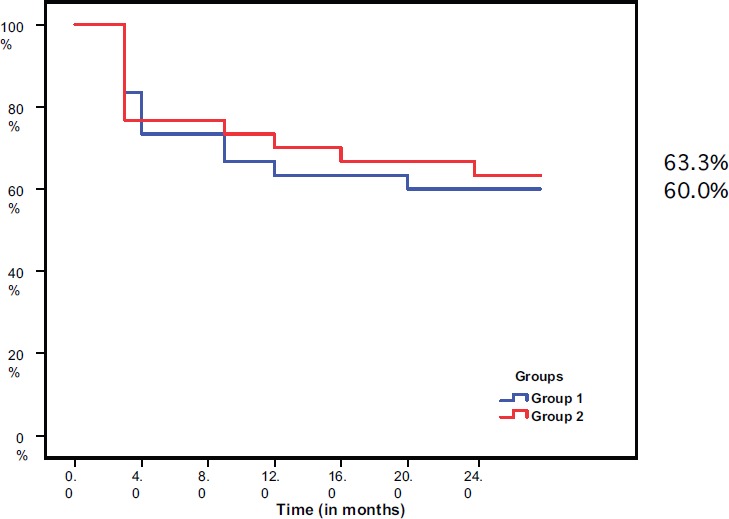
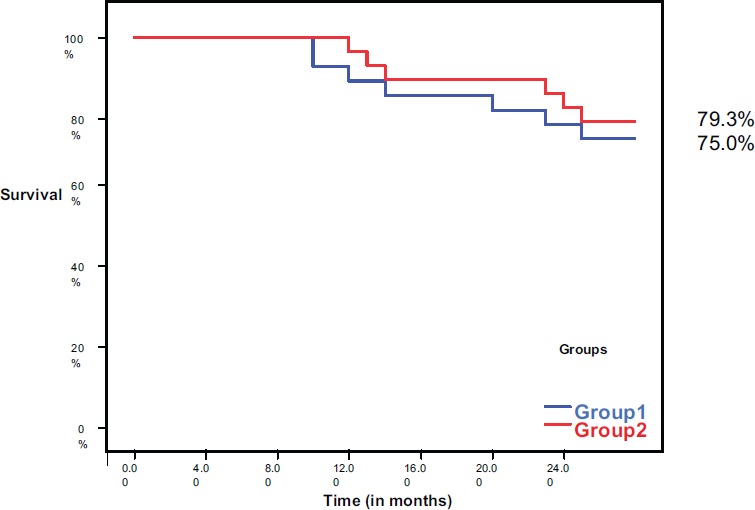
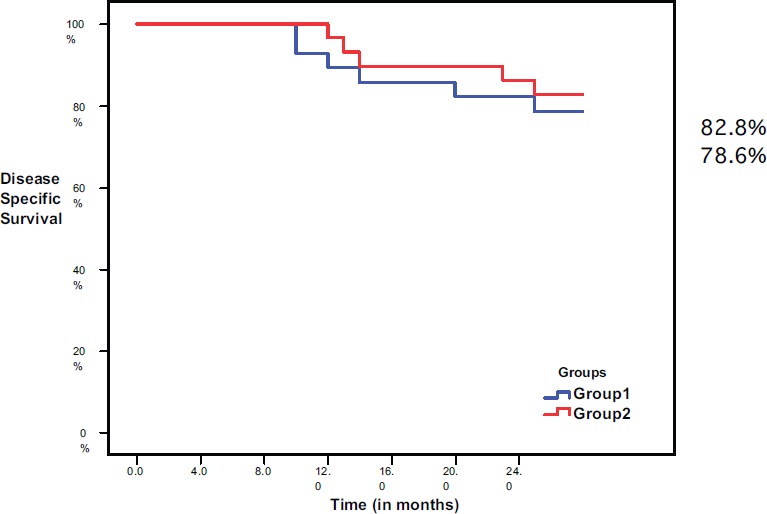
Results: The first assessment after the induction chemoradiotherapy showed that complete response was achieved in 73.3% of patients in group I and 76.7% of the patients in group II. After a median follow-up of 2 years, regional relapse occurred in 7.1% of patients in group I and 10.3% in group II. (p = 1). Distant metastases were detected in 17.9% of patient in group I and 13.8% in group II (p = 0.73). The 2-year disease-free survival was 60% in group I and 63.3% in group II (p = 0.79). The whole 2-year overall survival was 75% in group I and 79.3% in group II (p = 0.689). Radiation gastrointestinal (GI) acute toxicity was higher in group I than in group II (p = 0.001), while late GI radiation toxicity was comparable in both groups.
Conclusion: Treating the bladder only, without elective pelvic nodal irradiation, did not compromise pelvic control rate, but significantly decreased the acute radiation toxicity.
Keywords: bladder cancer; lymph nodes; radiotherapy; trimodality protocol.
Figures
References
-
- Yu Mc, Ross RK. Epidemiology of bladder cancer. In: Petrovich Z, Baert L, Bardy L, editors. Carcinoma of bladder. Berlin: Springer; 1998. pp. 1–13. 1998. - DOI
-
- Ferlay J, Bray F, Pisani P, et al. Lyon: IARC Press; 2004. GLOBOCAN 2002: Cancer incidence, mortality and prevalence worldwide. IARC Cancer Base No 5, version 2.0.
-
- Shipley WU, Kaufman DS, McDougal WS, et al. Cancer of the Bladder, Ureter and Renal Pelvis. In: DeVita VT Jr, Hellman S, Rosenberg SA, editors. Cancer Principles and Practice Oncology. 7. Philadelphia: Lippincott Williams & Wilkins; 2005. pp. 1168–92.
-
- Solsona E1, Climent MA, Iborra I, et al. Bladder preservation in selected patients with muscle-invasive bladder cancer by complete transurethral resection of the bladder plus systemic chemotherapy. Long term follow up of a phase II non randomized comparative trial with radical cystectomy. Eur Urol. 2009;55:911–921. doi: 10.1016/j.eururo.2008.08.027. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources