

Spinal gout: A review with case illustration
- PMID: 27900275
- PMCID: PMC5112347
- DOI: 10.5312/wjo.v7.i11.766
Spinal gout: A review with case illustration
Abstract
Aim: To summarize clinical presentations and treatment options of spinal gout in the literature from 2000 to 2014, and present theories for possible mechanism of spinal gout formation.
Methods: The authors reviewed 68 published cases of spinal gout, which were collected by searching "spinal gout" on PubMed from 2000 to 2014. The data were analyzed for clinical features, anatomical location of spinal gout, laboratory studies, imaging studies, and treatment choices.
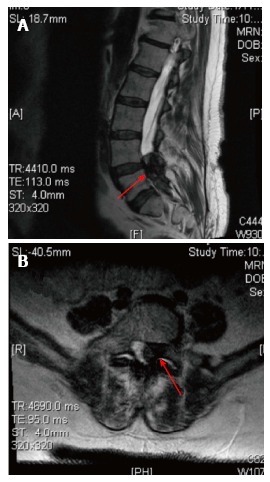
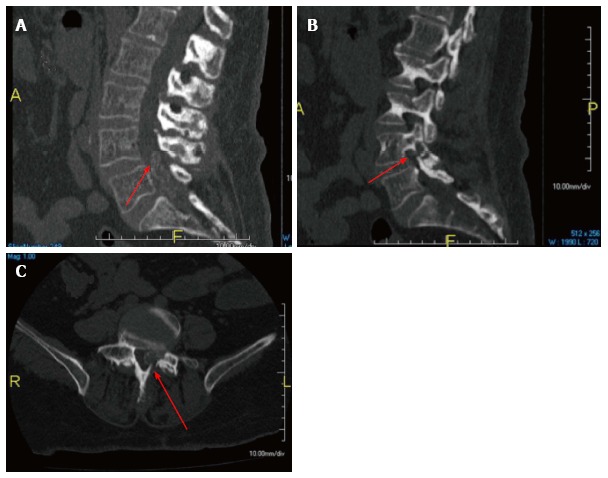
Results: Of the 68 patients reviewed, the most common clinical presentation was back or neck pain in 69.1% of patients. The most common laboratory study was elevated uric acid levels in 66.2% of patients. The most common diagnostic image finding was hypointense lesion of the gout tophi on the T1-weighted magnetic resonance imaging scan. The most common surgical treatment performed was a laminectomy in 51.5% and non-surgical treatment was performed in 29.4% of patients.
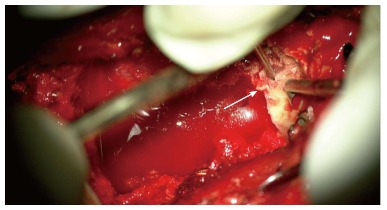
Conclusion: Spinal gout most commonly present as back or neck pain with majority of reported patients with elevated uric acid. The diagnosis of spinal gout is confirmed with the presence of negatively birefringent monosodium urate crystals in tissue. Treatment for spinal gout involves medication for the reduction of uric acid level and surgery if patient symptoms failed to respond to medical treatment.
Keywords: Gout; Monosodium urate; Spinal; Tophi.
Conflict of interest statement
Conflict-of-interest statement: None of the authors have any financial or other conflicts of interest that may bias the current study.
Figures

Similar articles
-
Understanding spinal gout: A comprehensive study of 88 cases and their clinical implications.J Craniovertebr Junction Spine. 2024 Apr-Jun;15(2):133-140. doi: 10.4103/jcvjs.jcvjs_166_23. Epub 2024 May 24. J Craniovertebr Junction Spine. 2024. PMID: 38957764 Free PMC article. Review.
-
A rare cause of back pain and radiculopathy - spinal tophi: a case report.J Med Case Rep. 2019 Jan 8;13(1):8. doi: 10.1186/s13256-018-1940-4. J Med Case Rep. 2019. PMID: 30626451 Free PMC article.
-
Endoscopic management of lumbar spinal tophaceous gout: six cases treated with percutaneous transforaminal (PTED) and interlaminar (PIED) discectomy and a literature review.Eur Spine J. 2025 May 17. doi: 10.1007/s00586-025-08849-2. Online ahead of print. Eur Spine J. 2025. PMID: 40382497 Review.
-
Unusual Dermatological Manifestations of Gout: Review of Literature and a Case Report.Plast Reconstr Surg Glob Open. 2015 Aug 10;3(7):e445. doi: 10.1097/GOX.0000000000000420. eCollection 2015 Jul. Plast Reconstr Surg Glob Open. 2015. PMID: 26301134 Free PMC article.
-
Gout involved the cervical disc and adjacent vertebral endplates misdiagnosed infectious spondylodiscitis on imaging: case report and literature review.BMC Musculoskelet Disord. 2019 Sep 14;20(1):425. doi: 10.1186/s12891-019-2813-8. BMC Musculoskelet Disord. 2019. PMID: 31521158 Free PMC article.
Cited by
-
Foraminal stenosis and radiculopathy secondary to tophaceous gout: illustrative case.J Neurosurg Case Lessons. 2023 Dec 25;6(26):CASE23298. doi: 10.3171/CASE23298. Print 2023 Dec 25. J Neurosurg Case Lessons. 2023. PMID: 38145559 Free PMC article.
-
Spinal gout with intervertebral foramen infiltration: A rare case perfectly mimicking degenerative lumbar disc disease.Exp Ther Med. 2023 Dec 18;27(2):66. doi: 10.3892/etm.2023.12354. eCollection 2024 Feb. Exp Ther Med. 2023. PMID: 38234610 Free PMC article.
-
A unique presentation of acute tophaceous gout in the lumbar spine causing cauda equina syndrome.Radiol Case Rep. 2023 Jul 14;18(9):3341-3345. doi: 10.1016/j.radcr.2023.06.070. eCollection 2023 Sep. Radiol Case Rep. 2023. PMID: 37520396 Free PMC article.
-
Lumbar spinal stenosis attributable to tophaceous gout: case report and review of the literature.Ther Clin Risk Manag. 2017 Sep 28;13:1287-1293. doi: 10.2147/TCRM.S145906. eCollection 2017. Ther Clin Risk Manag. 2017. PMID: 29033576 Free PMC article.
-
Case of lumbar spinal stenosis and chronic tophaceous gout.Surg Neurol Int. 2023 Aug 18;14:294. doi: 10.25259/SNI_504_2023. eCollection 2023. Surg Neurol Int. 2023. PMID: 37680922 Free PMC article.
References
-
- de Mello FM, Helito PV, Bordalo-Rodrigues M, Fuller R, Halpern AS. Axial gout is frequently associated with the presence of current tophi, although not with spinal symptoms. Spine (Phila Pa 1976) 2014;39:E1531–E1536. - PubMed
-
- Federman DG, Kravetz JD, Luciano RL, Brown JE. Gout: what a pain in the neck. Conn Med. 2012;76:143–146. - PubMed
-
- Sakamoto FA, Winalski CS, Rodrigues LC, Fernandes AR, Bortoletto A, Sundaram M. Radiologic case study. Orthopedics. 2012;35:353–437. - PubMed
-
- Kao MC, Huang SC, Chiu CT, Yao YT. Thoracic cord compression due to gout: a case report and literature review. J Formos Med Assoc. 2000;99:572–575. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
