

Survival and time-to-transplantation of peritoneal dialysis versus hemodialysis for end-stage renal disease patients: competing-risks regression model in a single Italian center experience
- PMID: 27900718
- PMCID: PMC5437127
- DOI: 10.1007/s40620-016-0366-6
Survival and time-to-transplantation of peritoneal dialysis versus hemodialysis for end-stage renal disease patients: competing-risks regression model in a single Italian center experience
Abstract
Aims: Despite several studies reporting similar outcomes for peritoneal dialysis (PD) and hemodialysis (HD), the former is underused worldwide, with a PD prevalence of 15% in Italy. In 2008, the Unit of Nephrology and Dialysis of the Healthcare Trust of the Autonomous Province of Trento implemented a successful PD program which has increased the proportion of PD incident patients from 7 to 47%. We aimed to assess the effect of this extensive use of PD by comparing HD and PD in terms of survival and time-to-transplantation.
Methods: A total of 334 HD and 153 PD incident patients were enrolled between January 2008 and December 2014. After screening for exclusion criteria and propensity score matching, 279 HD and 132 PD patients were analyzed. Survival and time-to-transplantation were assessed by competing-risks regression models, using death and transplantation as primary and competing events.
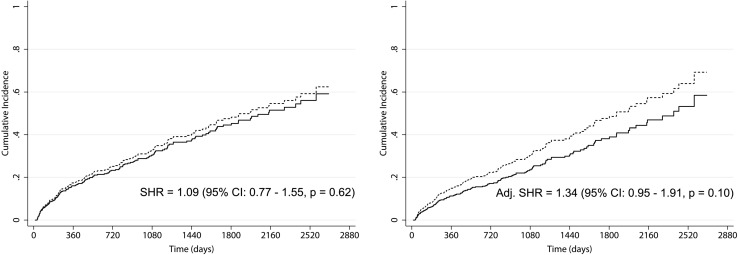
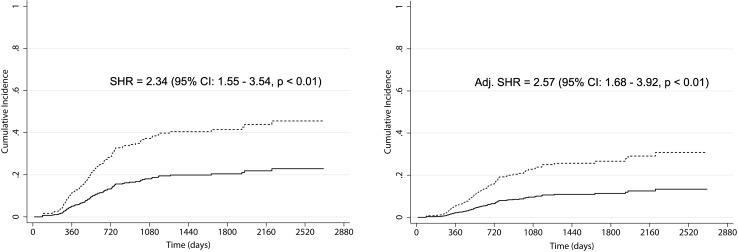
Results: Crude and adjusted regression models for survival revealed the absence of significant differences between HD and PD cumulative incidence functions (subhazard ratio: 1.09, p = 0.62 and 1.34, p = 0.10, respectively). Differently, crude and adjusted regression models for transplantation revealed a lower time-to-transplantation for PD versus HD patients (subhazard ratio: 2.34, p < 0.01, and 2.57, p < 0.01, respectively). The waiting time for placement in the transplant waiting list was longer in HD than PD patients (330 vs. 224 days, p < 0.01).
Conclusions: The extensive use of PD did not lead to any statistically significant difference in mortality. Furthermore, PD was associated with lower time to transplantation. PD may be a viable option for large-scale dialytic treatment in the advanced chronic kidney disease population.
Keywords: Advanced chronic kidney disease; Competing-risks model; Dialysis survival; Hemodialysis; Kidney transplantation; Peritoneal dialysis.
Conflict of interest statement
Conflict of interest
We have read and understood the Journal of Nephrology’s policy on disclosing conflicts of interest and declare that we have none.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. For this type of study formal consent is not required, since it is retrospective.
Figures
Similar articles
-
[REIN Report 2011--summary].Nephrol Ther. 2013 Sep;9 Suppl 1:S3-6. doi: 10.1016/S1769-7255(13)70036-1. Nephrol Ther. 2013. PMID: 24119584 French.
-
Survival of propensity matched incident peritoneal and hemodialysis patients in a United States health care system.Kidney Int. 2014 Nov;86(5):1016-22. doi: 10.1038/ki.2014.224. Epub 2014 Jul 2. Kidney Int. 2014. PMID: 24988066
-
Comparison of Subdural Hematoma Risk between Hemodialysis and Peritoneal Dialysis Patients with ESRD.Clin J Am Soc Nephrol. 2015 Jun 5;10(6):994-1001. doi: 10.2215/CJN.08140814. Epub 2015 Mar 30. Clin J Am Soc Nephrol. 2015. PMID: 25825482 Free PMC article.
-
Dialysis Modality and Mortality in the Elderly: A Meta-Analysis.Clin J Am Soc Nephrol. 2015 Jun 5;10(6):983-93. doi: 10.2215/CJN.05160514. Epub 2015 May 4. Clin J Am Soc Nephrol. 2015. PMID: 25941194 Free PMC article. Review.
-
Mortality studies comparing peritoneal dialysis and hemodialysis: what do they tell us?Kidney Int Suppl. 2006 Nov;(103):S3-11. doi: 10.1038/sj.ki.5001910. Kidney Int Suppl. 2006. PMID: 17080109 Review.
Cited by
-
Impact of the Type of Dialysis on Time to Transplantation: Is It Just a Matter of Immunity?J Clin Med. 2022 Feb 17;11(4):1054. doi: 10.3390/jcm11041054. J Clin Med. 2022. PMID: 35207326 Free PMC article.
-
Chronic kidney disease: prevalence and association with handgrip strength in a cross-sectional study.BMC Nephrol. 2021 Jul 2;22(1):246. doi: 10.1186/s12882-021-02452-5. BMC Nephrol. 2021. PMID: 34215205 Free PMC article.
-
Propensity Score-Matched Analysis of the Survival Benefit from Kidney Transplantation in Patients with End-Stage Renal Disease.J Clin Med. 2018 Oct 26;7(11):388. doi: 10.3390/jcm7110388. J Clin Med. 2018. PMID: 30373110 Free PMC article.
-
Propensity score matched mortality comparisons of peritoneal and in-centre haemodialysis: systematic review and meta-analysis.Nephrol Dial Transplant. 2020 Dec 4;35(12):2172-2182. doi: 10.1093/ndt/gfz278. Nephrol Dial Transplant. 2020. PMID: 31981353 Free PMC article.
-
Lessons Learnt during the COVID-19 Pandemic: For Patients with End-Stage Renal Disease, We Should Prioritize Home-Based Treatment and Telemedicine.Kidney Blood Press Res. 2021;46(1):11-16. doi: 10.1159/000512629. Epub 2021 Jan 29. Kidney Blood Press Res. 2021. PMID: 33517338 Free PMC article. Review.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
