

THE PATHOPHYSIOLOGY OF GEOGRAPHIC ATROPHY SECONDARY TO AGE-RELATED MACULAR DEGENERATION AND THE COMPLEMENT PATHWAY AS A THERAPEUTIC TARGET
- PMID: 27902638
- PMCID: PMC5424580
- DOI: 10.1097/IAE.0000000000001392
THE PATHOPHYSIOLOGY OF GEOGRAPHIC ATROPHY SECONDARY TO AGE-RELATED MACULAR DEGENERATION AND THE COMPLEMENT PATHWAY AS A THERAPEUTIC TARGET
Abstract
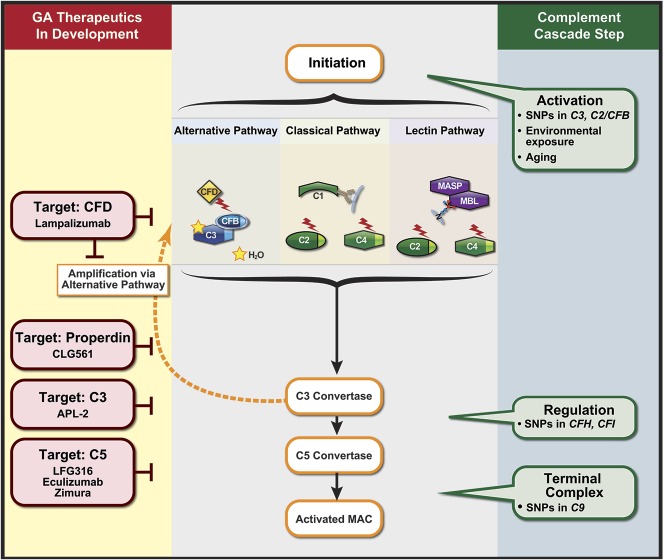
Purpose: Geographic atrophy (GA) is an advanced, vision-threatening form of age-related macular degeneration (AMD) affecting approximately five million individuals worldwide. To date, there are no approved therapeutics for GA treatment; however, several are in clinical trials. This review focuses on the pathophysiology of GA, particularly the role of complement cascade dysregulation and emerging therapies targeting the complement cascade.
Methods: Primary literature search on PubMed for GA, complement cascade in age-related macular degeneration. ClinicalTrials.gov was searched for natural history studies in GA and clinical trials of drugs targeting the complement cascade for GA.
Results: Cumulative damage to the retina by aging, environmental stress, and other factors triggers inflammation via multiple pathways, including the complement cascade. When regulatory components in these pathways are compromised, as with several GA-linked genetic risk factors in the complement cascade, chronic inflammation can ultimately lead to the retinal cell death characteristic of GA. Complement inhibition has been identified as a key candidate for therapeutic intervention, and drugs targeting the complement pathway are currently in clinical trials.
Conclusion: The complement cascade is a strategic target for GA therapy. Further research, including on natural history and genetics, is crucial to expand the understanding of GA pathophysiology and identify effective therapeutic targets.
Figures
References
-
- Holz FG, Strauss EC, Schmitz-Valckenberg S., Van Lookeren Campagne M. Geographic atrophy: clinical features and potential therapeutic approaches. Ophthalmology 2014;121:1079–1091. - PubMed
-
- Friedman DS, O'Colmain BJ, Munoz B, et al. Prevalence of age-related macular degeneration in the United States. Arch Ophthalmol 2004;122:564–572. - PubMed
-
- Rudnicka AR, Jarrar Z, Wormald R, et al. Age and gender variations in age-related macular degeneration prevalence in populations of European ancestry: a meta-analysis. Ophthalmology 2012;119:571–580. - PubMed
-
- Wong WL, Su X, Li X, et al. Global prevalence of age-related macular degeneration and disease burden projection for 2020 and 2040: a systematic review and meta-analysis. Lancet Glob Health 2014;2:e106–116. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
