

The Effect of Intravenous Immunoglobulin Combined with Corticosteroid on the Progression of Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis: A Meta-Analysis
- PMID: 27902746
- PMCID: PMC5130247
- DOI: 10.1371/journal.pone.0167120
The Effect of Intravenous Immunoglobulin Combined with Corticosteroid on the Progression of Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis: A Meta-Analysis
Abstract
Background: Intravenous immunoglobulin (IVIG) treatment is commonly used to treat Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) with controversial therapeutic effect.
Methods: We conducted a comprehensive meta-analysis through combining the published eligible studies to evaluate the effectiveness of IVIG on SJS and TEN treatment.
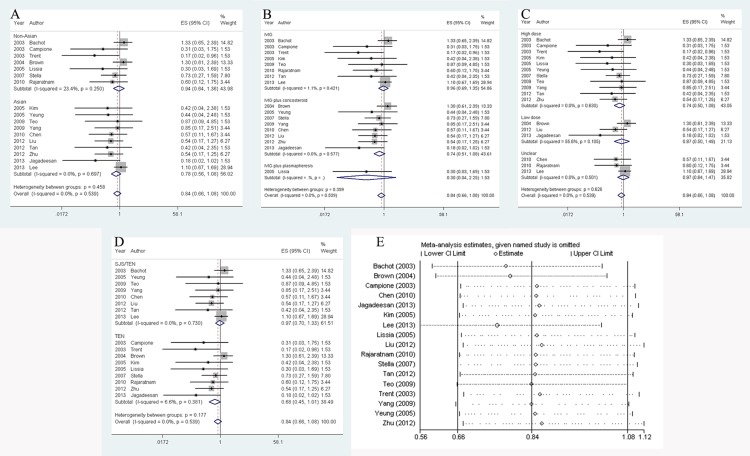
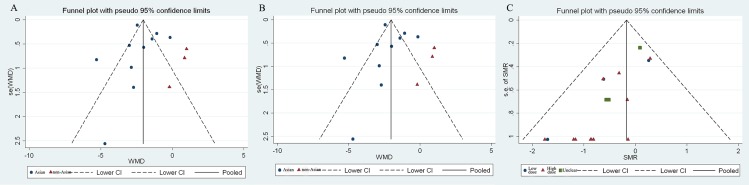
Results: A total of 26 studies were selected from public available databases. The combination of IVIG and corticosteroid markedly reduced the recovery time (by 1.63 days, 95% CI: 0.83-2.43, P < 0.001), compared with solo corticosteroid group. The favorable effects were greater in Asian (2.19, 95% CI: 1.41-2.97, P < 0.001), TEN (2.56, 95% CI: 0.35-4.77, P = 0.023) and high-dose IVIG treated individuals (1.78, 95% CI: 0.42-3.14, P = 0.010). The hospitalization length reduced by 3.19 days (95% CI: 0.08-6.30, P = 0.045), though the outcome was proven to be unstable. We found heterogeneities, which sources were probably regional factors. Besides, IVIG was inclined to decrease SJS/TEN mortality (SMR: 0.84, 95% CI: 0.66-1.08, P = 0.178). This impact was possibly more profound when patients were treated with high dose IVIG (SMR: 0.74, 95% CI: 0.50-1.08, P = 0.116), or when patients were diagnosed as TEN (SMR: 0.68, 95% CI: 0.45-1.01, P = 0.058).
Conclusions: Our current meta-analysis suggests that IVIG combined with corticosteroid could reduce recovery time for SJS and TEN. This effect is greater among Asian patients. Whereas, its impact on reducing mortality is not significant.
Conflict of interest statement
This article does not have any actual or potential conflict of interest including financial, personal or other relationships with other people or organizations.
Figures



Similar articles
-
Combination therapy of intravenous immunoglobulin and corticosteroid in the treatment of toxic epidermal necrolysis and Stevens-Johnson syndrome: a retrospective comparative study in China.Int J Dermatol. 2009 Oct;48(10):1122-8. doi: 10.1111/j.1365-4632.2009.04166.x. Int J Dermatol. 2009. PMID: 19775409
-
High-dose intravenous immunoglobulins in the treatment of Stevens-Johnson syndrome and toxic epidermal necrolysis in Chinese patients: a retrospective study of 82 cases.Eur J Dermatol. 2010 Nov-Dec;20(6):743-7. doi: 10.1684/ejd.2010.1077. Epub 2010 Oct 15. Eur J Dermatol. 2010. PMID: 20952352
-
Evaluation of Combination Therapy With Etanercept and Systemic Corticosteroids for Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis: A Multicenter Observational Study.J Allergy Clin Immunol Pract. 2022 May;10(5):1295-1304.e6. doi: 10.1016/j.jaip.2022.01.038. Epub 2022 Feb 4. J Allergy Clin Immunol Pract. 2022. PMID: 35131514
-
Intravenous immunoglobulin use in patients with toxic epidermal necrolysis and Stevens-Johnson syndrome.Am J Clin Dermatol. 2006;7(6):359-68. doi: 10.2165/00128071-200607060-00004. Am J Clin Dermatol. 2006. PMID: 17173470 Review.
-
Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis: A Concise Review with a Comprehensive Summary of Therapeutic Interventions Emphasizing Supportive Measures.Adv Ther. 2017 Jun;34(6):1235-1244. doi: 10.1007/s12325-017-0530-y. Epub 2017 Apr 24. Adv Ther. 2017. PMID: 28439852 Free PMC article. Review.
Cited by
-
Sutureless Amniotic Membrane (ProKera®) and Intravenous Immunoglobulin in the Management of Ocular Complications of Stevens-Johnson Syndrome-Toxic Epidermal Necrolysis Overlap.Cureus. 2021 Aug 8;13(8):e16989. doi: 10.7759/cureus.16989. eCollection 2021 Aug. Cureus. 2021. PMID: 34540392 Free PMC article.
-
Intravenous Immunoglobulin for the Rescue in Refractory Cutaneous Lupus.Indian Dermatol Online J. 2020 Sep 19;11(6):1003-1004. doi: 10.4103/idoj.IDOJ_82_20. eCollection 2020 Nov-Dec. Indian Dermatol Online J. 2020. PMID: 33344358 Free PMC article. No abstract available.
-
Amniotic membrane grafting for acute ocular involvement in Stevens-Johnson syndrome: Review of perioperative considerations, surgical techniques, and outcomes.Indian J Ophthalmol. 2025 Apr 1;73(4):553-562. doi: 10.4103/IJO.IJO_1238_24. Epub 2025 Mar 27. Indian J Ophthalmol. 2025. PMID: 40146142 Free PMC article. Review.
-
Stevens-Johnson syndrome triggered by phenytoin in a patient with type 2 diabetes and seizures.Explor Res Clin Soc Pharm. 2025 Jun 13;19:100624. doi: 10.1016/j.rcsop.2025.100624. eCollection 2025 Sep. Explor Res Clin Soc Pharm. 2025. PMID: 40662055 Free PMC article.
-
Acute and chronic ocular outcomes in SJS/TEN patients treated with oral ciclosporin vs intravenous immunoglobulin.Front Med (Lausanne). 2024 Aug 19;11:1398506. doi: 10.3389/fmed.2024.1398506. eCollection 2024. Front Med (Lausanne). 2024. PMID: 39224611 Free PMC article.
References
-
- Bastuji-Garin S, Rzany B, Stern RS, Shear NH, Naldi L, Roujeau JC. Clinical classification of cases of toxic epidermal necrolysis, Stevens-Johnson syndrome, and erythema multiforme. Arch Dermatol. 1993;129(1): 92–6. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
