

Type 2 Diabetes Mellitus and Cancer: The Role of Pharmacotherapy
- PMID: 27903154
- PMCID: PMC5455318
- DOI: 10.1200/JCO.2016.67.4044
Type 2 Diabetes Mellitus and Cancer: The Role of Pharmacotherapy
Abstract
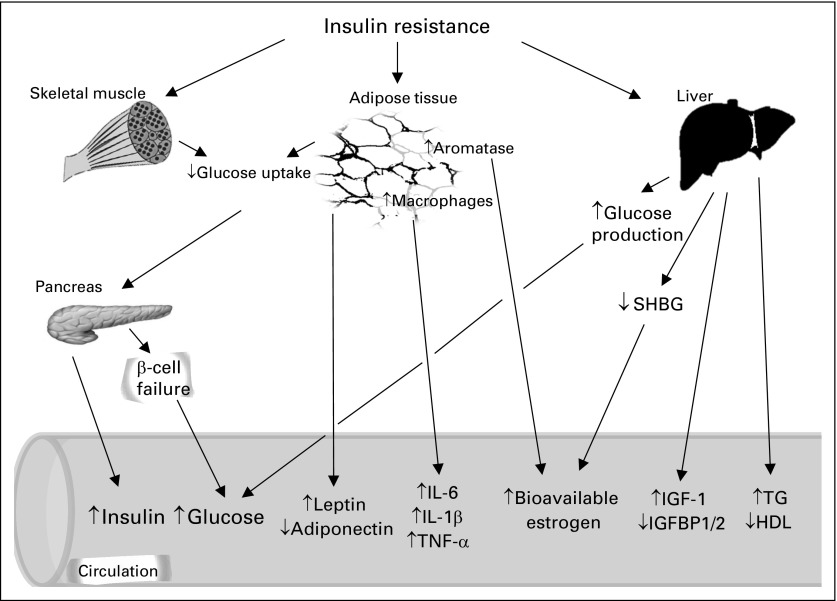
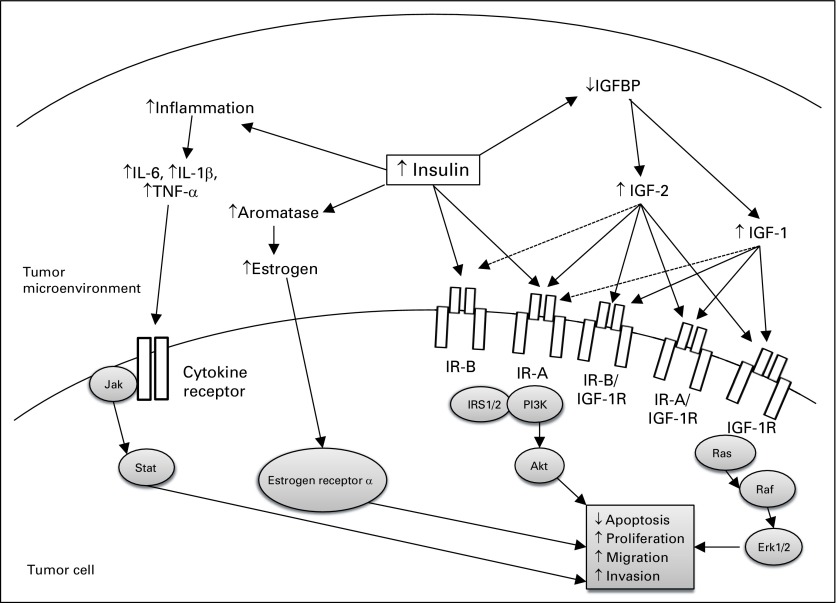
Purpose Type 2 diabetes mellitus (T2DM) is becoming increasingly prevalent worldwide. Epidemiologic data suggest that T2DM is associated with an increased incidence and mortality from many cancers. The purpose of this review is to discuss the links between diabetes and cancer, the effects of various antidiabetic medications on cancer incidence and mortality, and the effects of anticancer therapies on diabetes. Design This study is a review of preclinical and clinical data regarding the effects of antidiabetic medications on cancer incidence and mortality and the effects of anticancer therapies on glucose homeostasis. Results T2DM is associated with an increased risk and greater mortality from many cancer types. Metformin use has been associated with a decrease in cancer incidence and mortality, and there are many ongoing randomized trials investigating the effects of metformin on cancer-related outcomes. However, data regarding the association of other antidiabetes medications with cancer incidence and mortality are conflicting. Glucocorticoids, hormone-based therapies, inhibitors that target the phosphatidylinositol 3-kinase-Akt-mammalian target of rapamycin pathway, and insulin-like growth factor 1 receptor-targeted therapy have been associated with high rates of hyperglycemia. These agents mediate their deleterious metabolic effects by reducing insulin secretion and increasing insulin resistance in peripheral tissues. Conclusion Studies must be performed to optimize cancer screening strategies in individuals with T2DM. A greater understanding of the mechanisms that link diabetes and cancer are needed to identify targets for therapy in individuals with diabetes who develop cancer. Data from clinical studies are needed to further elucidate the effects of antidiabetic medications on cancer incidence and progression. As several anticancer therapies alter glucose homeostasis, physicians need to be aware of these potential effects. Careful patient screening and monitoring during treatment with these agents is necessary.
Conflict of interest statement
Authors’ disclosures of potential conflicts of interest are found in the article online at
Figures
References
-
- Alberti KG. Screening and diagnosis of prediabetes: Where are we headed? Diabetes Obes Metab. 2007;9(Suppl 1):12–16. - PubMed
-
- Tsilidis KK, Kasimis JC, Lopez DS, et al. Type 2 diabetes and cancer: Umbrella review of meta-analyses of observational studies. BMJ. 2015;350:g7607. - PubMed
-
- Harding JL, Shaw JE, Peeters A, et al. Cancer risk among people with type 1 and type 2 diabetes: Disentangling true associations, detection bias, and reverse causation. Diabetes Care. 2015;38:264–270. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
