

Clinical, physiologic, and radiographic factors contributing to development of hypoxemia in moderate to severe COPD: a cohort study
- PMID: 27903260
- PMCID: PMC5131397
- DOI: 10.1186/s12890-016-0331-0
Clinical, physiologic, and radiographic factors contributing to development of hypoxemia in moderate to severe COPD: a cohort study
Abstract
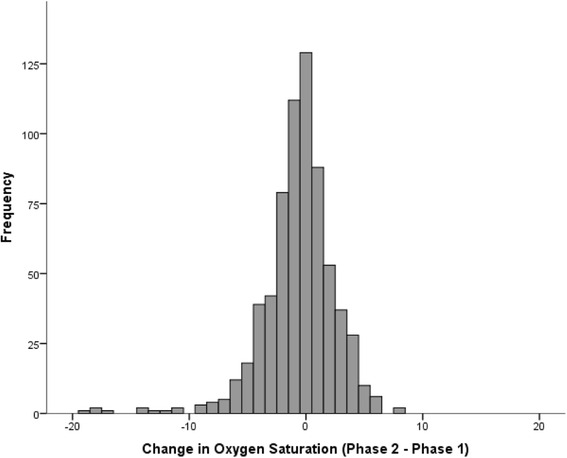
Background: Hypoxemia is a major complication of COPD and is a strong predictor of mortality. We previously identified independent risk factors for the presence of resting hypoxemia in the COPDGene cohort. However, little is known about characteristics that predict onset of resting hypoxemia in patients who are normoxic at baseline. We hypothesized that a combination of clinical, physiologic, and radiographic characteristics would predict development of resting hypoxemia after 5-years of follow-up in participants with moderate to severe COPD METHODS: We analyzed 678 participants with moderate-to-severe COPD recruited into the COPDGene cohort who completed baseline and 5-year follow-up visits and who were normoxic by pulse oximetry at baseline. Development of resting hypoxemia was defined as an oxygen saturation ≤88% on ambient air at rest during follow-up. Demographic and clinical characteristics, lung function, and radiographic indices were analyzed with logistic regression models to identify predictors of the development of hypoxemia.
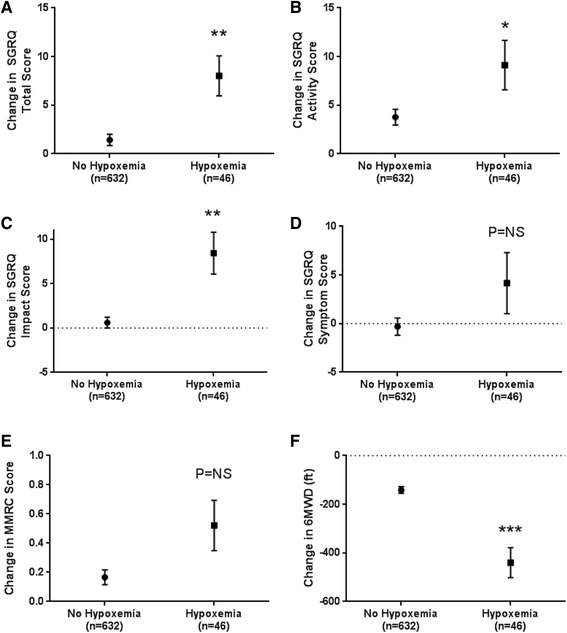
Results: Forty-six participants (7%) developed resting hypoxemia at follow-up. Enrollment at Denver (OR 8.30, 95%CI 3.05-22.6), lower baseline oxygen saturation (OR 0.70, 95%CI 0.58-0.85), self-reported heart failure (OR 6.92, 95%CI 1.56-30.6), pulmonary artery (PA) enlargement on computed tomography (OR 2.81, 95%CI 1.17-6.74), and prior severe COPD exacerbation (OR 3.31, 95%CI 1.38-7.90) were independently associated with development of resting hypoxemia. Participants who developed hypoxemia had greater decline in 6-min walk distance and greater 5-year decline in quality of life compared to those who remained normoxic at follow-up.
Conclusions: Development of clinically significant hypoxemia over a 5-year span is associated with comorbid heart failure, PA enlargement and severe COPD exacerbation. Further studies are needed to determine if treatments targeting these factors can prevent new onset hypoxemia.
Trial registration: COPDGene is registered at ClinicalTrials.gov: NCT00608764 (Registration Date: January 28, 2008).
Figures

References
-
- Zielinski J, MacNee W, Wedzicha J, Ambrosino N, Braghiroli A, Dolensky J, Howard P, Gorzelak K, Lahdensuo A, Strom K, et al. Causes of death in patients with COPD and chronic respiratory failure. Monaldi Arch Chest Dis. 1997;52(1):43–47. - PubMed
-
- Antonucci R, Berton E, Huertas A, Laveneziana P, Palange P. Exercise physiology in COPD. Monaldi Arch Chest Dis. 2003;59(2):134–139. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
- KL2 TR001419/TR/NCATS NIH HHS/United States
- R01 HL089897/HL/NHLBI NIH HHS/United States
- S10 OD018526/OD/NIH HHS/United States
- P30 ES005605/ES/NIEHS NIH HHS/United States
- U01 HL089897/HL/NHLBI NIH HHS/United States
- R01 HL094635/HL/NHLBI NIH HHS/United States
- R01 HL116931/HL/NHLBI NIH HHS/United States
- R01 HL089856/HL/NHLBI NIH HHS/United States
- K01 HL118714/HL/NHLBI NIH HHS/United States
- R01 HL116473/HL/NHLBI NIH HHS/United States
- U01 HL089856/HL/NHLBI NIH HHS/United States
- K08 HL123940/HL/NHLBI NIH HHS/United States
- UL1 TR001417/TR/NCATS NIH HHS/United States
- R01 HL125583/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
