

Standardized flow cytometry for highly sensitive MRD measurements in B-cell acute lymphoblastic leukemia
- PMID: 27903527
- PMCID: PMC5291958
- DOI: 10.1182/blood-2016-07-726307
Standardized flow cytometry for highly sensitive MRD measurements in B-cell acute lymphoblastic leukemia
Abstract
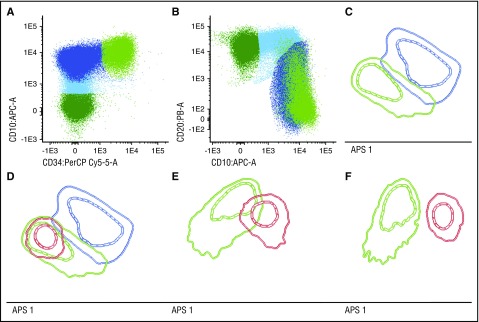
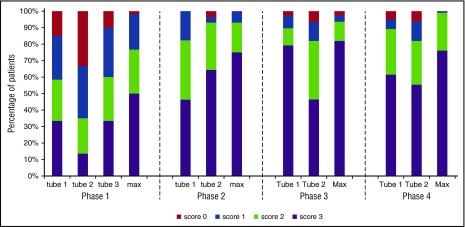
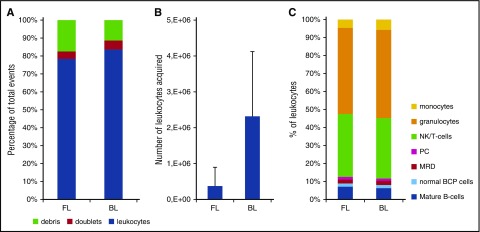
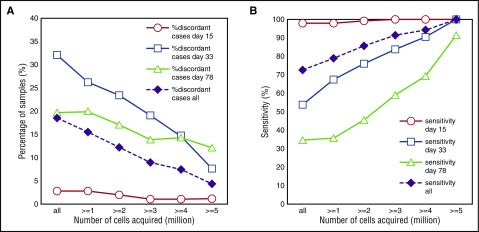
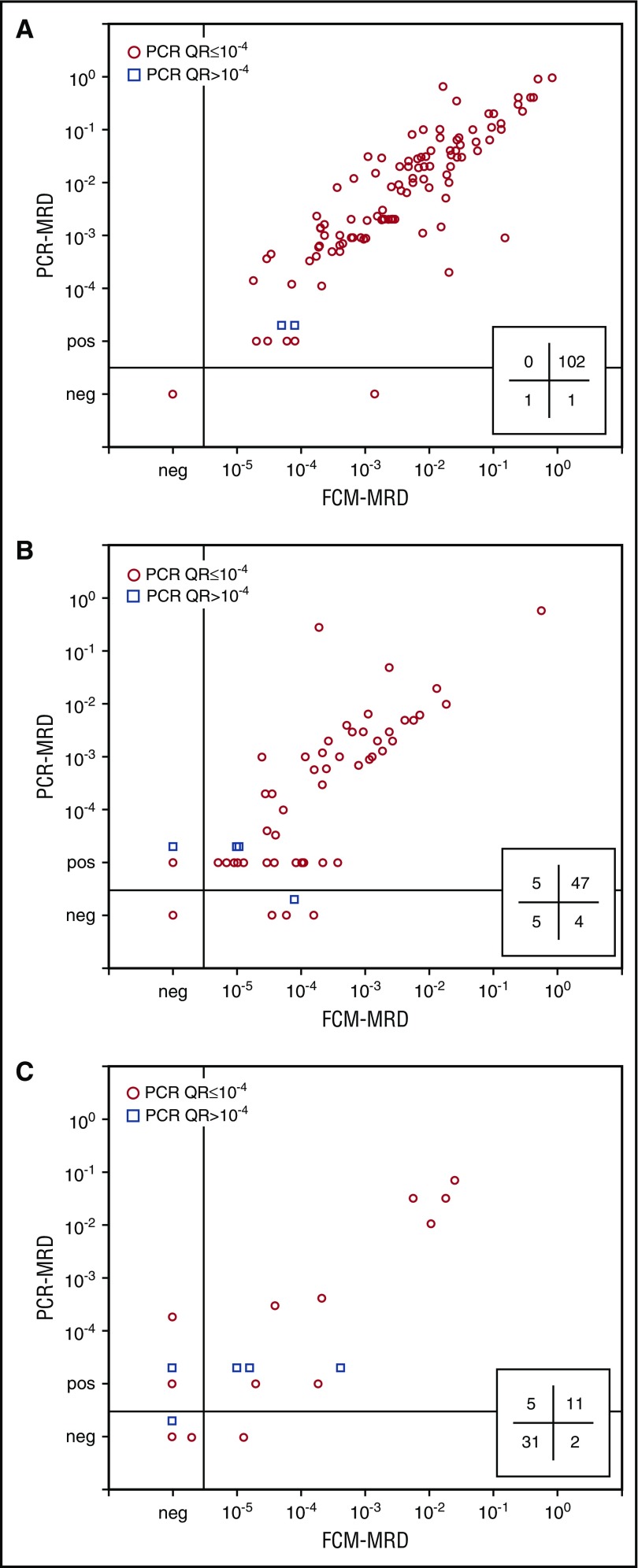
A fully-standardized EuroFlow 8-color antibody panel and laboratory procedure was stepwise designed to measure minimal residual disease (MRD) in B-cell precursor (BCP) acute lymphoblastic leukemia (ALL) patients with a sensitivity of ≤10-5, comparable to real-time quantitative polymerase chain reaction (RQ-PCR)-based MRD detection via antigen-receptor rearrangements. Leukocyte markers and the corresponding antibodies and fluorochromes were selected based on their contribution in separating BCP-ALL cells from normal/regenerating BCP cells in multidimensional principal component analyses. After 5 multicenter design-test-evaluate-redesign phases with a total of 319 BCP-ALL patients at diagnosis, two 8-color antibody tubes were selected, which allowed separation between normal and malignant BCP cells in 99% of studied patients. These 2 tubes were tested with a new erythrocyte bulk-lysis protocol allowing acquisition of high cell numbers in 377 bone marrow follow-up samples of 178 BCP-ALL patients. Comparison with RQ-PCR-based MRD data showed a clear positive relation between the percentage concordant cases and the number of cells acquired. For those samples with >4 million cells acquired, concordant results were obtained in 93% of samples. Most discordances were clarified upon high-throughput sequencing of antigen-receptor rearrangements and blind multicenter reanalysis of flow cytometric data, resulting in an unprecedented concordance of 98% (97% for samples with MRD < 0.01%). In conclusion, the fully standardized EuroFlow BCP-ALL MRD strategy is applicable in >98% of patients with sensitivities at least similar to RQ-PCR (≤10-5), if sufficient cells (>4 × 106, preferably more) are evaluated.
© 2017 by The American Society of Hematology.
Figures
Comment in
-
A reproducible strategy for analysis of minimal residual disease measured by Standardized multiparametric flow cytometry in b acute lymphoblastic leukemia.Cytometry B Clin Cytom. 2019 Jan;96(1):12-15. doi: 10.1002/cyto.b.21720. Epub 2018 Oct 24. Cytometry B Clin Cytom. 2019. PMID: 30353651 No abstract available.
References
-
- Flohr T, Schrauder A, Cazzaniga G, et al. ; International BFM Study Group (I-BFM-SG). Minimal residual disease-directed risk stratification using real-time quantitative PCR analysis of immunoglobulin and T-cell receptor gene rearrangements in the international multicenter trial AIEOP-BFM ALL 2000 for childhood acute lymphoblastic leukemia. Leukemia. 2008;22(4):771-782. - PubMed
-
- van der Velden VH, Cazzaniga G, Schrauder A, et al. ; European Study Group on MRD detection in ALL (ESG-MRD-ALL). Analysis of minimal residual disease by Ig/TCR gene rearrangements: guidelines for interpretation of real-time quantitative PCR data. Leukemia. 2007;21(4):604-611. - PubMed
-
- van der Velden VH, van Dongen JJ. MRD detection in acute lymphoblastic leukemia patients using Ig/TCR gene rearrangements as targets for real-time quantitative PCR. Methods Mol Biol. 2009;538:115-150. - PubMed
-
- Basso G, Veltroni M, Valsecchi MG, et al. Risk of relapse of childhood acute lymphoblastic leukemia is predicted by flow cytometric measurement of residual disease on day 15 bone marrow. J Clin Oncol. 2009;27(31):5168-5174. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
