

High Structural Stress and Presence of Intraluminal Thrombus Predict Abdominal Aortic Aneurysm 18F-FDG Uptake: Insights From Biomechanics
- PMID: 27903534
- PMCID: PMC5113243
- DOI: 10.1161/CIRCIMAGING.116.004656
High Structural Stress and Presence of Intraluminal Thrombus Predict Abdominal Aortic Aneurysm 18F-FDG Uptake: Insights From Biomechanics
Abstract
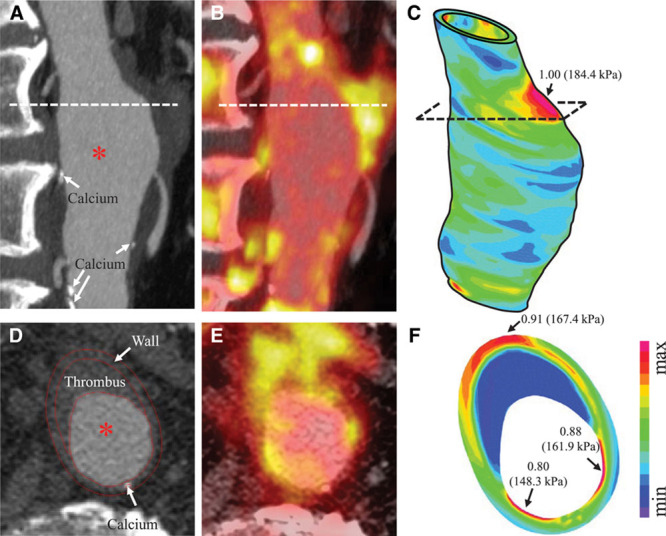
Background: Abdominal aortic aneurysm (AAA) wall inflammation and mechanical structural stress may influence AAA expansion and lead to rupture. We hypothesized a positive correlation between structural stress and fluorine-18-labeled 2-deoxy-2-fluoro-d-glucose (18F-FDG) positron emission tomography-defined inflammation. We also explored the influence of computed tomography-derived aneurysm morphology and composition, including intraluminal thrombus, on both variables.
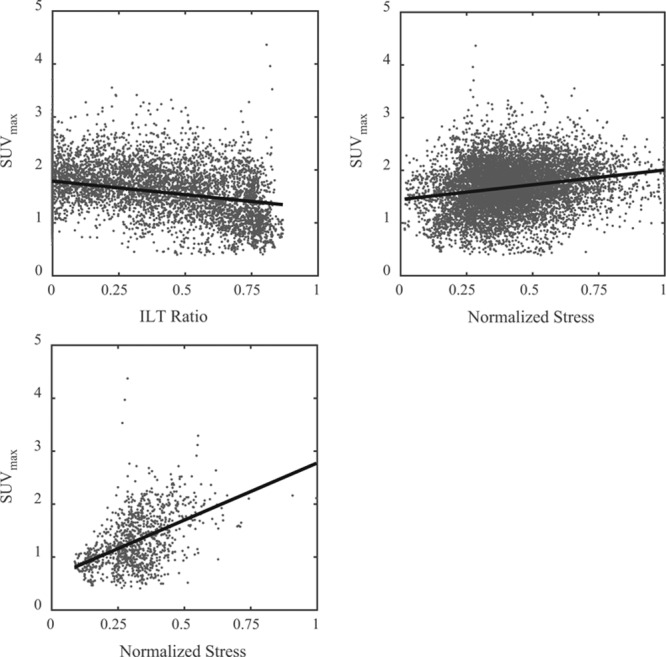
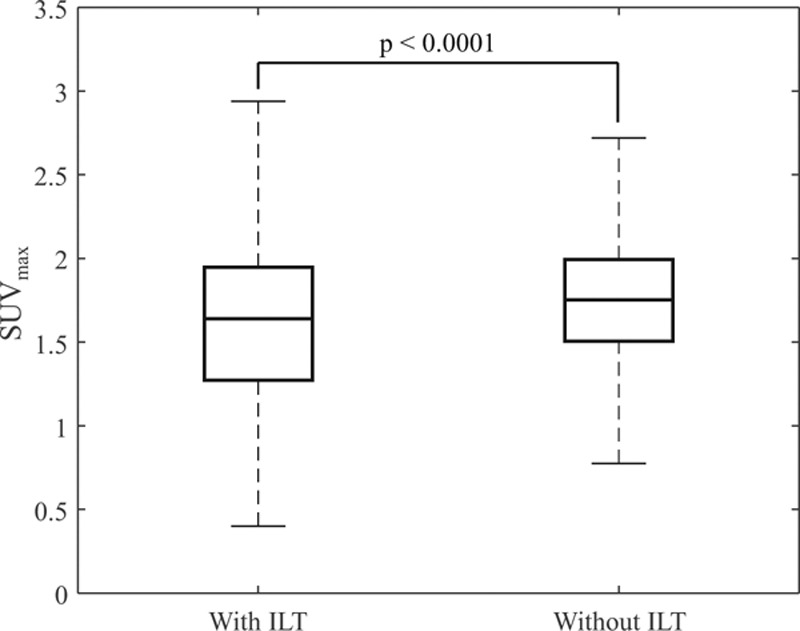
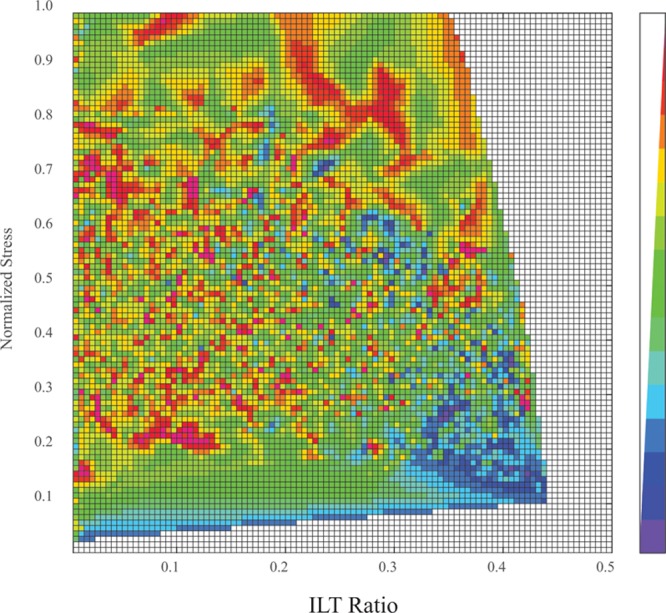
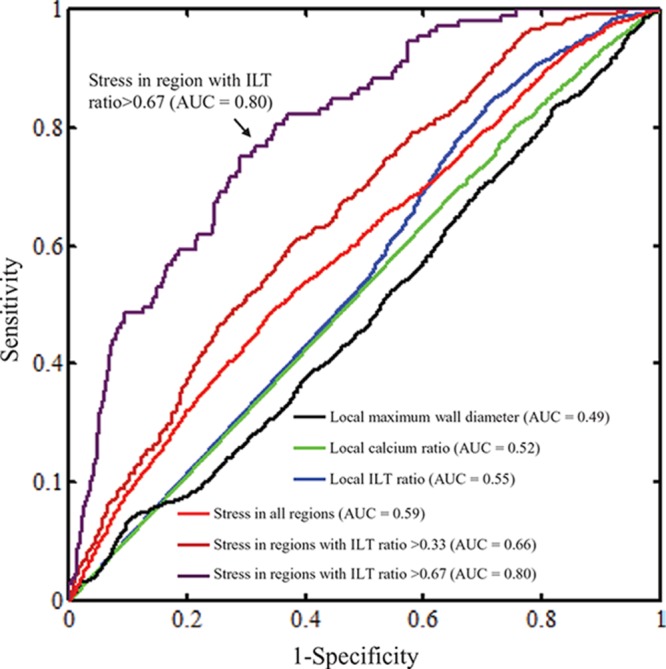
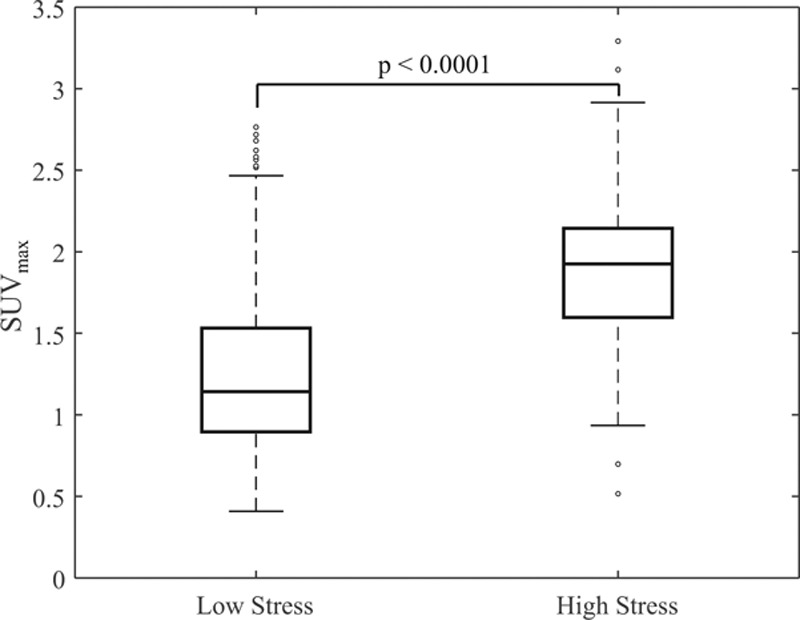
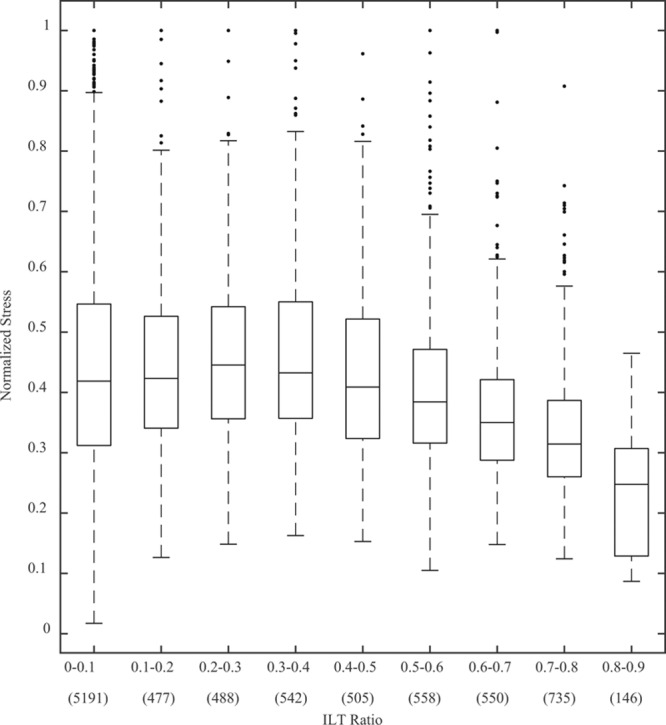
Methods and results: Twenty-one patients (19 males) with AAAs below surgical threshold (AAA size was 4.10±0.54 cm) underwent 18F-FDG positron emission tomography and contrast-enhanced computed tomography imaging. Structural stresses were calculated using finite element analysis. The relationship between maximum aneurysm 18F-FDG standardized uptake value within aortic wall and wall structural stress, patient clinical characteristics, aneurysm morphology, and compositions was explored using a hierarchical linear mixed-effects model. On univariate analysis, local aneurysm diameter, thrombus burden, extent of calcification, and structural stress were all associated with 18F-FDG uptake (P<0.05). AAA structural stress correlated with 18F-FDG maximum standardized uptake value (slope estimate, 0.552; P<0.0001). Multivariate linear mixed-effects analysis revealed an important interaction between structural stress and intraluminal thrombus in relation to maximum standardized uptake value (fixed effect coefficient, 1.68 [SE, 0.10]; P<0.0001). Compared with other factors, structural stress was the best predictor of inflammation (receiver-operating characteristic curve area under the curve =0.59), with higher accuracy seen in regions with high thrombus burden (area under the curve =0.80). Regions with both high thrombus burden and high structural stress had higher 18F-FDG maximum standardized uptake value compared with regions with high thrombus burdens but low stress (median [interquartile range], 1.93 [1.60-2.14] versus 1.14 [0.90-1.53]; P<0.0001).
Conclusions: Increased aortic wall inflammation, demonstrated by 18F-FDG positron emission tomography, was observed in AAA regions with thick intraluminal thrombus subjected to high mechanical stress, suggesting a potential mechanistic link underlying aneurysm inflammation.
Keywords: abdominal aortic aneurysm; fluorodeoxyglucose F18; inflammation; mechanical stress; positron-emission tomography; thrombosis.
© 2016 The Authors.
Figures
Comment in
-
Positron Emission Tomography Fluorine-18-Labeled 2-Deoxy-2-Fluoro-d-Glucose Tells a Complicated Story in the Aortic Aneurysm Wall.Circ Cardiovasc Imaging. 2016 Nov;9(11):e005689. doi: 10.1161/CIRCIMAGING.116.005689. Circ Cardiovasc Imaging. 2016. PMID: 27903546 Free PMC article. No abstract available.
Similar articles
-
On the influence of wall calcification and intraluminal thrombus on prediction of abdominal aortic aneurysm rupture.J Vasc Surg. 2018 Apr;67(4):1234-1246.e2. doi: 10.1016/j.jvs.2017.05.086. Epub 2017 Sep 9. J Vasc Surg. 2018. PMID: 28899569
-
Inflammation as a Predictor of Abdominal Aortic Aneurysm Growth and Rupture: A Systematic Review of Imaging Biomarkers.Eur J Vasc Endovasc Surg. 2016 Sep;52(3):333-42. doi: 10.1016/j.ejvs.2016.05.002. Epub 2016 Jun 6. Eur J Vasc Endovasc Surg. 2016. PMID: 27283346
-
Multifactorial relationship between 18F-fluoro-deoxy-glucose positron emission tomography signaling and biomechanical properties in unruptured aortic aneurysms.Circ Cardiovasc Imaging. 2014 Jan;7(1):82-91. doi: 10.1161/CIRCIMAGING.112.000415. Epub 2013 Nov 4. Circ Cardiovasc Imaging. 2014. PMID: 24190906
-
Feasibility of Assessing Inflammation in Asymptomatic Abdominal Aortic Aneurysms With Integrated 18F-Fluorodeoxyglucose Positron Emission Tomography/Magnetic Resonance Imaging.Eur J Vasc Endovasc Surg. 2020 Mar;59(3):464-471. doi: 10.1016/j.ejvs.2019.04.004. Epub 2019 Nov 8. Eur J Vasc Endovasc Surg. 2020. PMID: 31708339
-
Biomechanical Indices for Rupture Risk Estimation in Abdominal Aortic Aneurysms.J Endovasc Ther. 2017 Apr;24(2):254-261. doi: 10.1177/1526602816680088. Epub 2016 Nov 21. J Endovasc Ther. 2017. PMID: 27872318 Review.
Cited by
-
Imaging Predictive Factors of Abdominal Aortic Aneurysm Growth.J Clin Med. 2021 Apr 28;10(9):1917. doi: 10.3390/jcm10091917. J Clin Med. 2021. PMID: 33925046 Free PMC article. Review.
-
Positron Emission Tomography Fluorine-18-Labeled 2-Deoxy-2-Fluoro-d-Glucose Tells a Complicated Story in the Aortic Aneurysm Wall.Circ Cardiovasc Imaging. 2016 Nov;9(11):e005689. doi: 10.1161/CIRCIMAGING.116.005689. Circ Cardiovasc Imaging. 2016. PMID: 27903546 Free PMC article. No abstract available.
-
Monocytes and macrophages in abdominal aortic aneurysm.Nat Rev Cardiol. 2017 Aug;14(8):457-471. doi: 10.1038/nrcardio.2017.52. Epub 2017 Apr 13. Nat Rev Cardiol. 2017. PMID: 28406184 Review.
-
Prospect of positron emission tomography for abdominal aortic aneurysm risk stratification.J Nucl Cardiol. 2021 Oct;28(5):2272-2282. doi: 10.1007/s12350-021-02616-8. Epub 2021 May 11. J Nucl Cardiol. 2021. PMID: 33977372 Free PMC article. Review.
-
Molecular Imaging of Aortic Aneurysm and Its Translational Power for Clinical Risk Assessment.Front Med (Lausanne). 2022 Apr 15;9:814123. doi: 10.3389/fmed.2022.814123. eCollection 2022. Front Med (Lausanne). 2022. PMID: 35492343 Free PMC article. Review.
References
-
- Kent KC. Clinical practice. Abdominal aortic aneurysms. N Engl J Med. 2014;371:2101–2108. doi: 10.1056/NEJMcp1401430. - PubMed
-
- Ashton HA, Buxton MJ, Day NE, Kim LG, Marteau TM, Scott RA, Thompson SG, Walker NM Multicentre Aneurysm Screening Study Group. The Multicentre Aneurysm Screening Study (MASS) into the effect of abdominal aortic aneurysm screening on mortality in men: a randomised controlled trial. Lancet. 2002;360:1531–1539. - PubMed
-
- Powell JT, Brown LC, Greenhalgh RM, Thompson SG. The rupture rate of large abdominal aortic aneurysms: is this modified by anatomical suitability for endovascular repair? Ann Surg. 2008;247:173–179. doi: 10.1097/SLA.0b013e3181557d2a. - PubMed
-
- Shah PK. Inflammation, metalloproteinases, and increased proteolysis: an emerging pathophysiological paradigm in aortic aneurysm. Circulation. 1997;96:2115–2117. - PubMed
-
- Courtois A, Nusgens BV, Hustinx R, Namur G, Gomez P, Somja J, Defraigne JO, Delvenne P, Michel JB, Colige AC, Sakalihasan N. 18F-FDG uptake assessed by PET/CT in abdominal aortic aneurysms is associated with cellular and molecular alterations prefacing wall deterioration and rupture. J Nucl Med. 2013;54:1740–1747. doi: 10.2967/jnumed.112.115873. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
