

Beyond a single pathway: combination therapy in pulmonary arterial hypertension
- PMID: 27903663
- PMCID: PMC9487558
- DOI: 10.1183/16000617.0085-2016
Beyond a single pathway: combination therapy in pulmonary arterial hypertension
Abstract
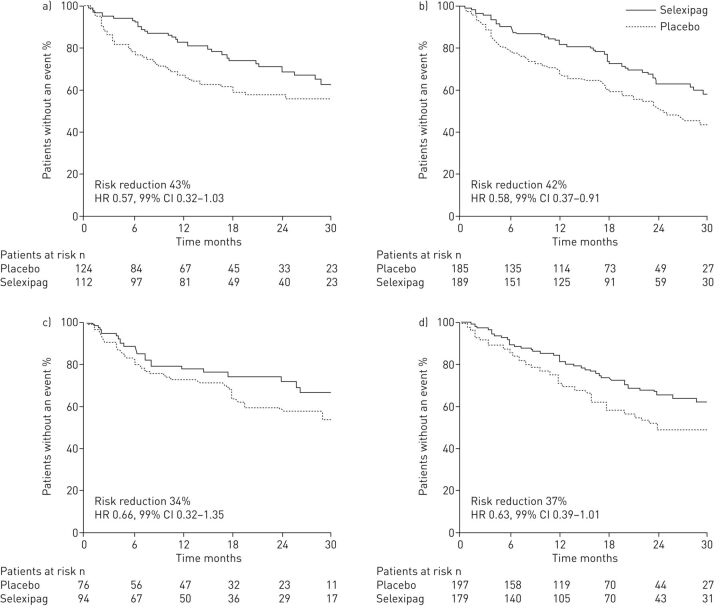
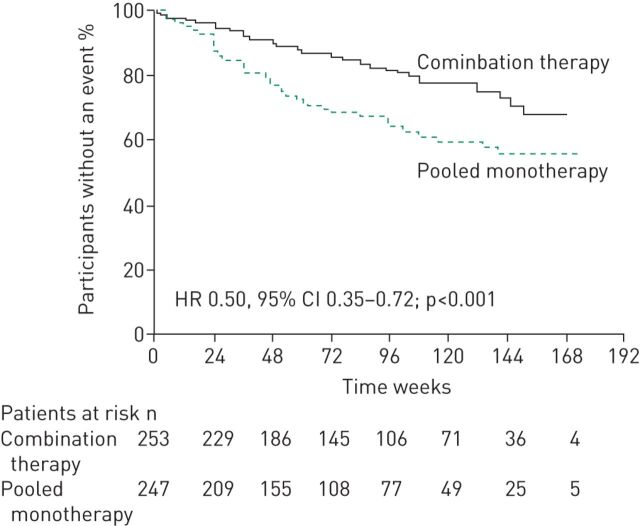
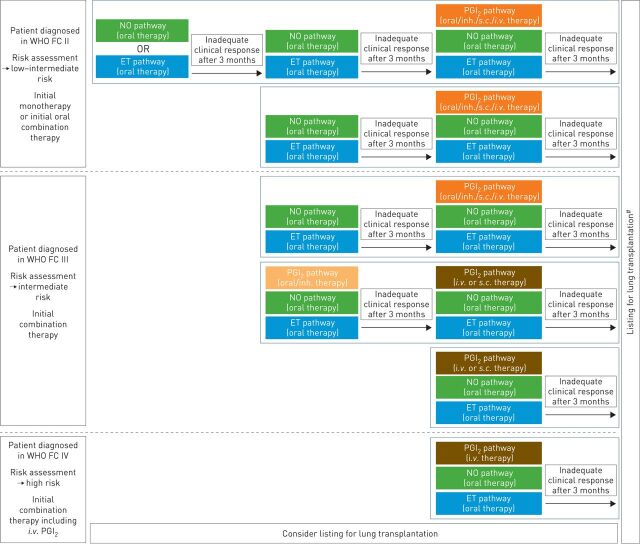
There is a strong rationale for combining therapies to simultaneously target three of the key pathways implicated in the pathogenesis of pulmonary arterial hypertension (PAH). Evidence to support this strategy is growing, and a number of studies have demonstrated that combination therapy, administered as either a sequential or an initial regimen, can improve long-term outcomes in PAH. Dual combination therapy with a phosphodiesterase-5 inhibitor and an endothelin receptor antagonist is the most widely utilised combination regimen. However, some patients fail to achieve their treatment goals on dual therapy and may benefit from the addition of a third drug. The use of triple therapy in clinical practice was previously reserved for patients with severe disease due to the need for parenteral administration of prostanoids. Although triple therapy with parenteral prostanoids plays a key role in the management of severe PAH, the approval of oral therapies that target the prostacyclin pathway means that all three pathways can now be targeted with oral drugs at an earlier disease stage. Furthermore, there is evidence demonstrating that this approach can delay disease progression. Based on the evidence available, it is becoming increasingly clear that all PAH patients should be offered the benefits of combination therapy.
Copyright ©ERS 2016.
Conflict of interest statement
Editorial comment in
Conflict of interest: Disclosures can be found alongside this article at
Figures

References
-
- Cihlar T, Fordyce M. Current status and prospects of HIV treatment. Curr Opin Virol 2016; 18: 50–56. - PubMed
-
- Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the Use of Antiretroviral Agents in HIV-1-infected Adults and Adolescents. Department of Health and Human Services. http://aidsinfo.nih.gov/contentfiles/lvguidelines/AdultandAdolescentGL.pdf Date last accessed: July 2016. Date last updated: July 14, 2016.
-
- Vaduganathan M, Mentz RJ, Greene SJ, et al. Combination decongestion therapy in hospitalized heart failure: loop diuretics, mineralocorticoid receptor antagonists and vasopressin antagonists. Expert Rev Cardiovasc Ther 2015; 13: 799–809. - PubMed
-
- Cole GD, Patel SJ, Zaman N, et al. “Triple therapy” of heart failure with angiotensin-converting enzyme inhibitor, beta-blocker, and aldosterone antagonist may triple survival time: shouldn't we tell patients? JACC Heart Fail 2014; 2: 545–548. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical