

Survival outcomes and surgical intervention of small intestinal neuroendocrine tumors: a population based retrospective study
- PMID: 27903960
- PMCID: PMC5354882
- DOI: 10.18632/oncotarget.13632
Survival outcomes and surgical intervention of small intestinal neuroendocrine tumors: a population based retrospective study
Abstract
Background: Small intestinal neuroendocrine tumors (SiNETs) without distant metastasis typically behave in an indolent manner, but there can be heterogeneity. We aimed to define the survival outcomes and impacts of surgical intervention.
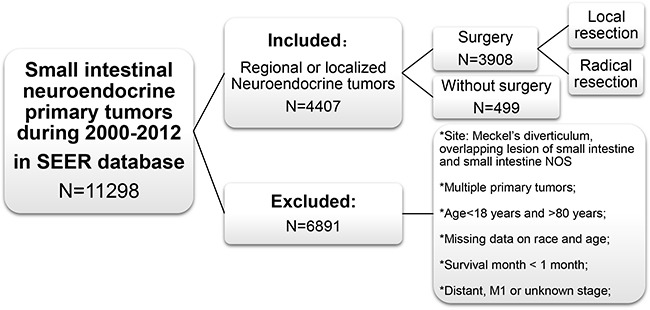
Methods: A retrospective cohort study was conducted by using data from the Surveillance, Epidemiology, and End Results (SEER) database. Clinicopathologic features were analyzed in 4407 patients between 2000 and 2012. The cancer specific survival (CSS) was calculated by the Kaplan-Meier method. Multivariable Cox regression models with hazard ratios (HRs) were constructed to analyze survival outcomes and risk factors.
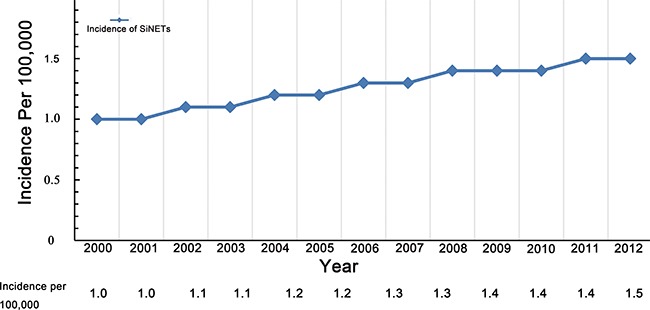
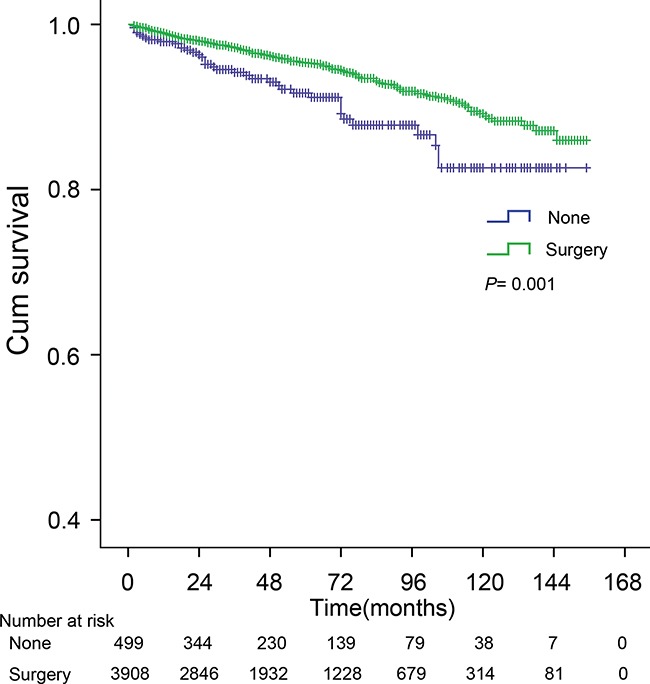
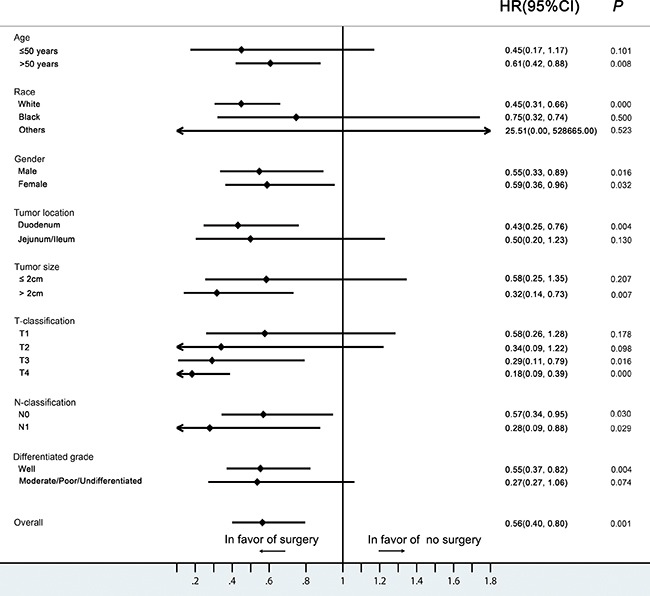
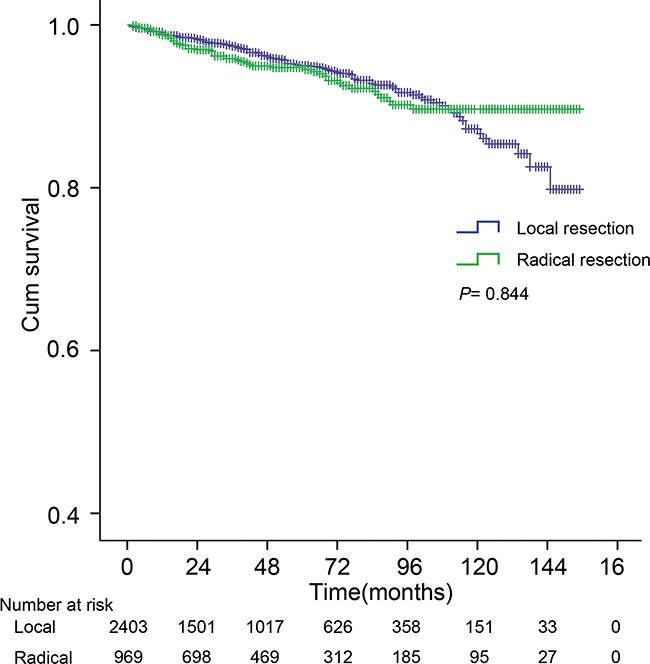
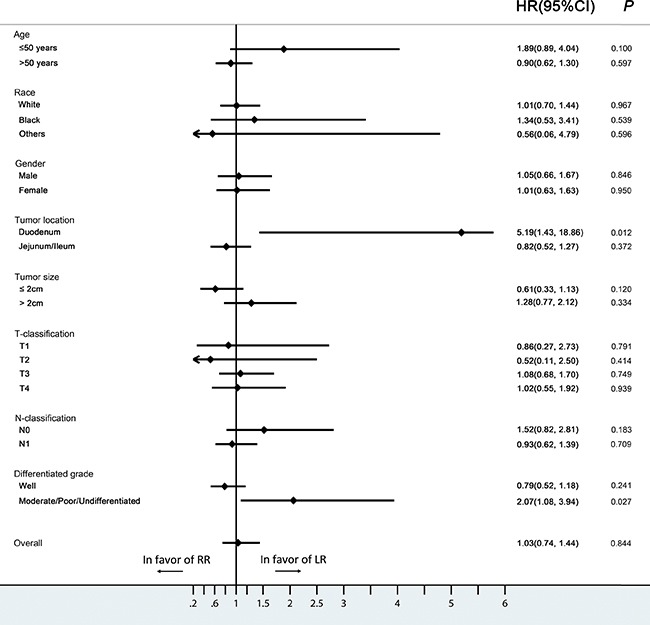
Results: The adjusted incidence of early SiNETs is 1.3/100,000. Tumors are most commonly located in the ileum and are small (≤ 2 cm). The 5-year and 10-year CSS rates were 95.0% and 88.5%, respectively. Age > 50 years, large tumor size (> 2cm), poor differentiation, advanced T classification, and absence of surgical treatment were independent predictors of poor survival. Stratified analysis indicated that surgery significantly improved survival in patients that were white (HR, 0.45), > 50 years old (HR, 0.61), had duodenal tumors (HR, 0.43), large tumors (> 2cm) (HR, 0.32), advanced T classification (T3: HR, 0.29; T4: HR, 0.18) or well differentiation (HR, 0.55). There was no significant survival difference between local resection and radical resection (P =0.884).
Conclusions: Early SiNETs have a favorable prognosis. Surgical resection may improve outcomes, particularly in older patients and those with large tumors. More aggressive resections couldn't improve outcomes.
Keywords: SEER; neuroendocrine tumors; prognostic factors; small intestine; surgical management.
Conflict of interest statement
None declared
Figures
References
-
- Modlin IM, Oberg K, Chung DC, Jensen RT, de Herder WW, Thakker RV, Caplin M, G Delle Fave, Kaltsas GA, Krenning EP, Moss SF, Nilsson O, Rindi G, Salazar R, Ruszniewski P, Sundin A. Gastroenteropancreatic neuroendocrine tumours. Lancet Oncol. 2008;9:61–72. - PubMed
-
- Oberndorfer S. Karzinoide Tumoren des Dunndarms. Frankfurt Z Pathol. 1907;1:426–432.
-
- Modlin IM, Shapiro MD, Kidd M, Eick G. Siegfried oberndorfer and the evolution of carcinoid disease. Arch Surg. 2007;142:187–197. - PubMed
-
- Kloppel G, Perren A, Heitz PU. The gastroenteropancreatic neuroendocrine cell system and its tumors: the WHO classification. Ann N Y Acad Sci. 2004;1014:13–27. - PubMed
-
- Yao JC, Hassan M, Phan A, Dagohoy C, Leary C, Mares JE, Abdalla EK, Fleming JB, Vauthey JN, Rashid A, Evans DB. One hundred years after “carcinoid”: epidemiology of and prognostic factors for neuroendocrine tumors in 35,825 cases in the United States. J Clin Oncol. 2008;26:3063–3072. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
