

Novel risk models for early detection and screening of ovarian cancer
- PMID: 27903971
- PMCID: PMC5352196
- DOI: 10.18632/oncotarget.13648
Novel risk models for early detection and screening of ovarian cancer
Abstract
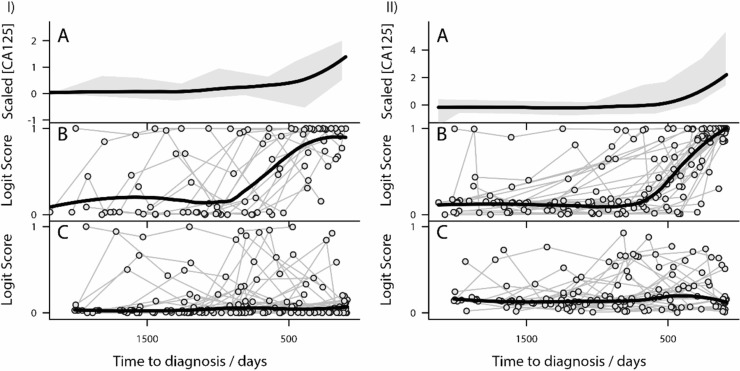
Purpose: Ovarian cancer (OC) is the most lethal gynaecological cancer. Early detection is required to improve patient survival. Risk estimation models were constructed for Type I (Model I) and Type II (Model II) OC from analysis of Protein Z, Fibronectin, C-reactive protein and CA125 levels in prospectively collected samples from the United Kingdom Collaborative Trial of Ovarian Cancer Screening (UKCTOCS).
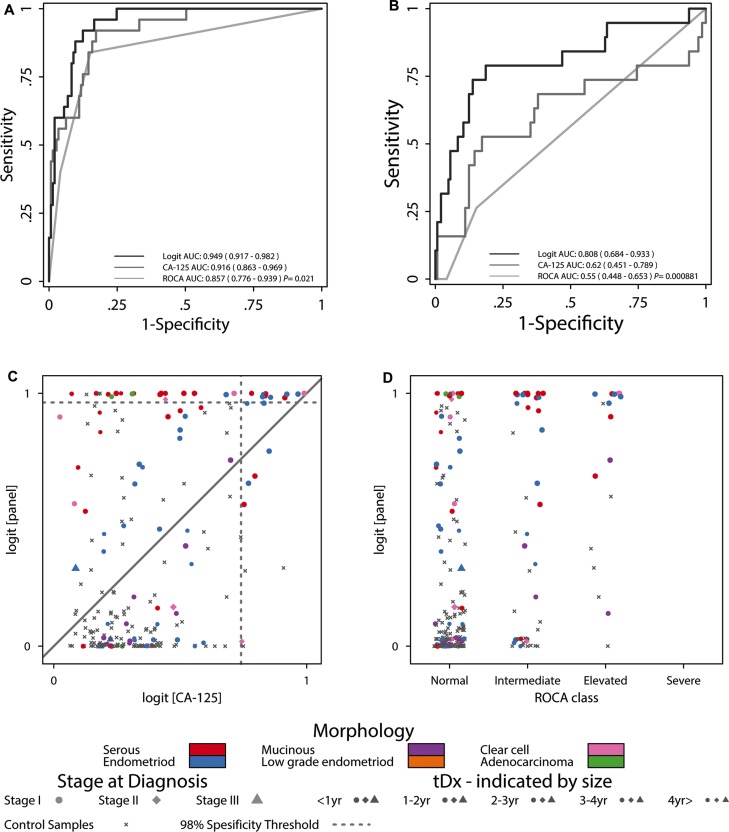
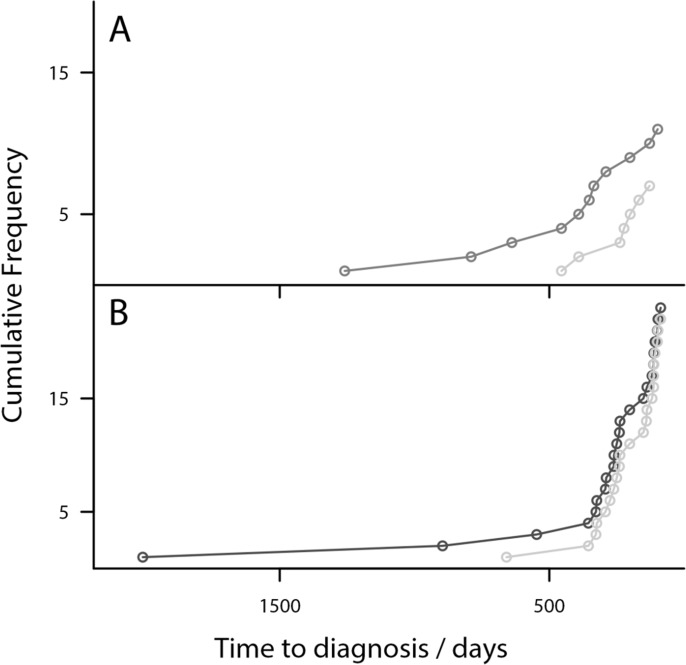
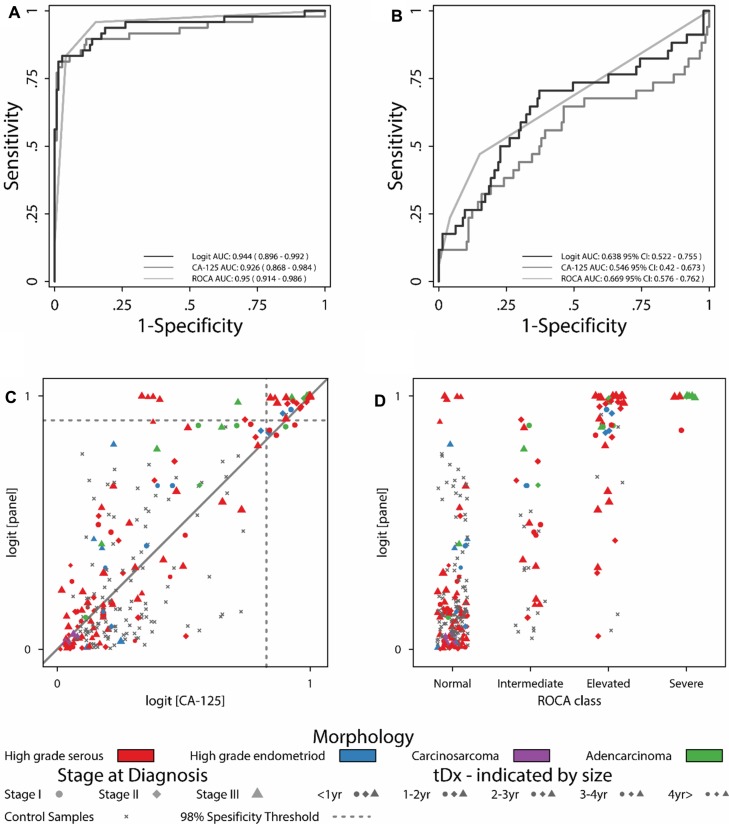
Results: Model I identifies cancers earlier than CA125 alone, with a potential lead time of 3-4 years. Model II detects a number of high grade serous cancers at an earlier stage (Stage I/II) than CA125 alone, with a potential lead time of 2-3 years and assigns high risk to patients that the ROCA Algorithm classified as normal.
Materials and methods: This nested case control study included 418 individual serum samples serially collected from 49 OC cases and 31 controls up to six years pre-diagnosis. Discriminatory logit models were built combining the ELISA results for candidate proteins with CA125 levels.
Conclusions: These models have encouraging sensitivities for detecting pre-clinical ovarian cancer, demonstrating improved sensitivity compared to CA125 alone. In addition we demonstrate how the models improve on ROCA for some cases and outline their potential future use as clinical tools.
Keywords: UKCTOCS; early detection; logit; ovarian cancer; risk estimation.
Conflict of interest statement
The authors declare the following potential conflicts of interest. Both I.J. and U.M. have a financial interest through UCL Business and Abcodia Ltd in the commercial use of UKCTOCS samples. I.J. is a Non-Executive Director and Consultant to Abcodia Ltd and a Director of Women's Health Specialists Ltd. I.J. is a co-inventor of the ROCA algorithm and has rights to a potential royalty stream from the owners of the algorithm MGH and QMUL universities.
Figures
References
-
- Hüttenhain R, Soste M, Selevsek N, Röst H, Sethi A, Carapito C, Farrah T, Deutsch EW, Kusebauch U, Moritz RL, Niméus-Malmström E, Rinner O, Aebersold R. Reproducible Quantification of Cancer-Associated Proteins in Body Fluids Using Targeted Proteomics. Sci Transl Med. 2012;4:142ra194. - PMC - PubMed
-
- CRUK Ovarian Cancer Survival statistics
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
