

CURRENT CONCEPTS AND TREATMENT OF PATELLOFEMORAL COMPRESSIVE ISSUES
- PMID: 27904792
- PMCID: PMC5095942
CURRENT CONCEPTS AND TREATMENT OF PATELLOFEMORAL COMPRESSIVE ISSUES
Abstract
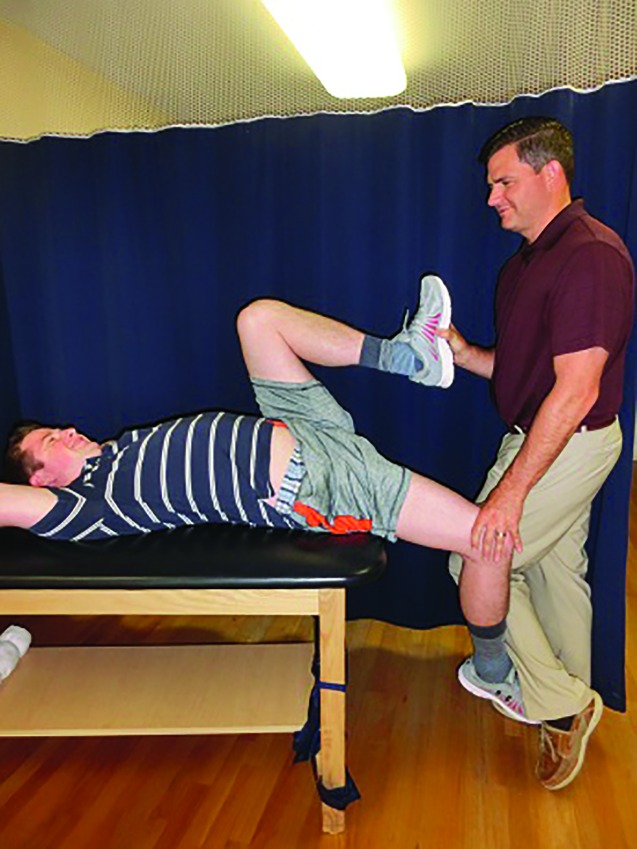
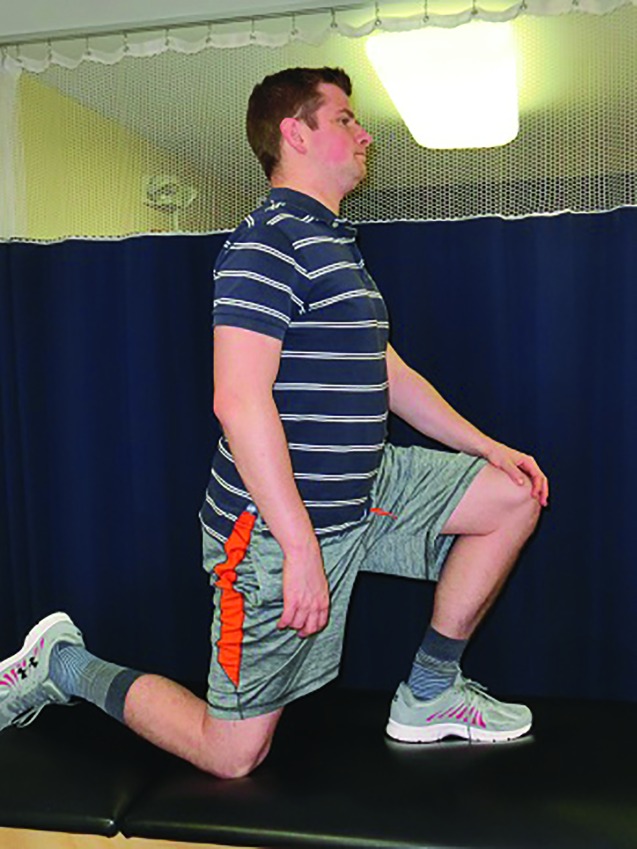
Patellofemoral disorders, commonly encountered in sports and orthopedic rehabilitation settings, may result from dysfunction in patellofemoral joint compression. Osseous and soft tissue factors, as well as the mechanical interaction of the two, contribute to increased patellofemoral compression and pain. Treatment of patellofemoral compressive issues is based on identification of contributory impairments. Use of reliable tests and measures is essential in detecting impairments in hip flexor, quadriceps, iliotibial band, hamstrings, and gastrocnemius flexibility, as well as in joint mobility, myofascial restrictions, and proximal muscle weakness. Once relevant impairments are identified, a combination of manual techniques, instrument-assisted methods, and therapeutic exercises are used to address the impairments and promote functional improvements. The purpose of this clinical commentary is to describe the clinical presentation, contributory considerations, and interventions to address patellofemoral joint compressive issues.
Keywords: Flexibility; knee; patellofemoral compression; patellofemoral pain.
Figures




References
-
- Kannus P Aho H Jarvinen M Niittymaki S. Computerized recording of visits to an outpatient sports clinic. Am J Sports Med. 1987;15(1):79-85. - PubMed
-
- Blond L Hansen L. Patellofemoral pain syndrome in athletes: a 5.7-year retrospective follow-up study of 250 athletes. Acta Orthop Belg. 1998;64(4):393-400. - PubMed
-
- Baquie P Brukner P. Injuries presenting to an Australian sports medicine centre: a 12-month study. Clin J Sport Med. 1997;7(1):28-31. - PubMed
-
- Sherman SL Plackis AC Nuelle CW. Patellofemoral anatomy and biomechanics. Clin Sports Med. 2014;33(3):389-401. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources