

One-third of Hips After Periacetabular Osteotomy Survive 30 Years With Good Clinical Results, No Progression of Arthritis, or Conversion to THA
- PMID: 27905061
- PMCID: PMC5339143
- DOI: 10.1007/s11999-016-5169-5
One-third of Hips After Periacetabular Osteotomy Survive 30 Years With Good Clinical Results, No Progression of Arthritis, or Conversion to THA
Abstract
Background: Since its first description in 1984, periacetabular osteotomy (PAO) has become an accepted treatment for hip dysplasia. The 30-year survivorship with this procedure has not been reported. Because these patients are often very young at the time of surgery, long-term followup and identification of factors associated with poor outcome could help to improve patient selection.
Questions/purposes: Looking at the initial group of patients with hip dysplasia undergoing PAO at the originator's institution, we asked: (1) What is the cumulative 30-year survival rate free from conversion to THA, radiographic progression of osteoarthritis, and/or a Merle d'Aubigné-Postel score < 15? (2) Did hip function improve and pain decrease? (3) Did radiographic osteoarthritis progress? (4) What are the factors associated with one or more of the three endpoints: THA, radiographic progression of osteoarthritis, and/or Merle d'Aubigné-Postel score < 15?
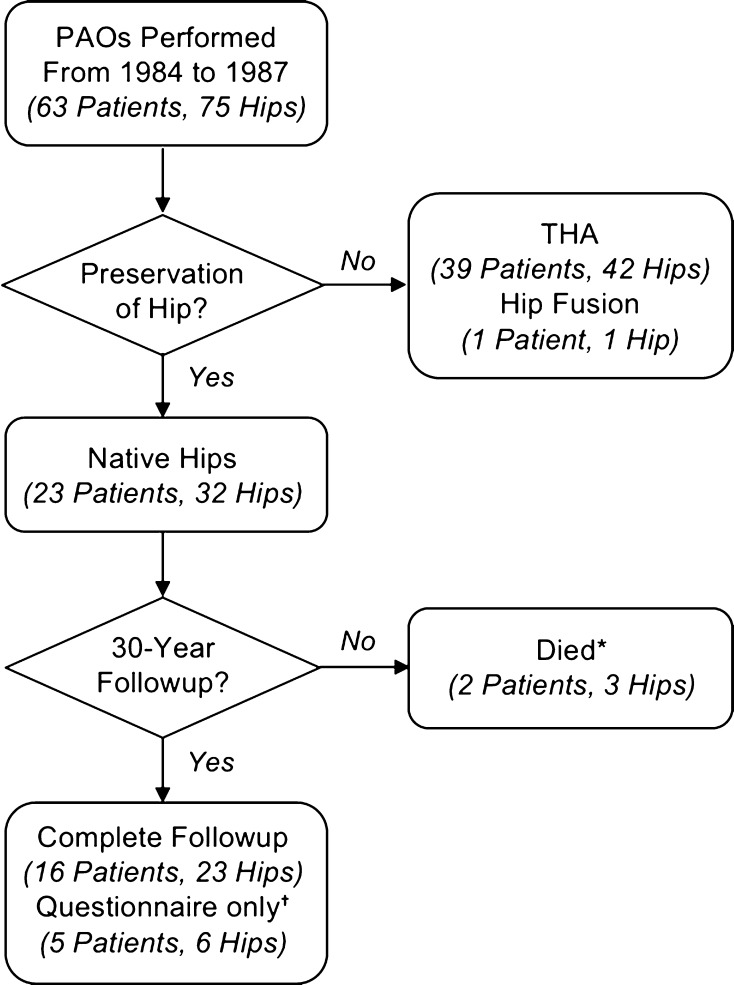
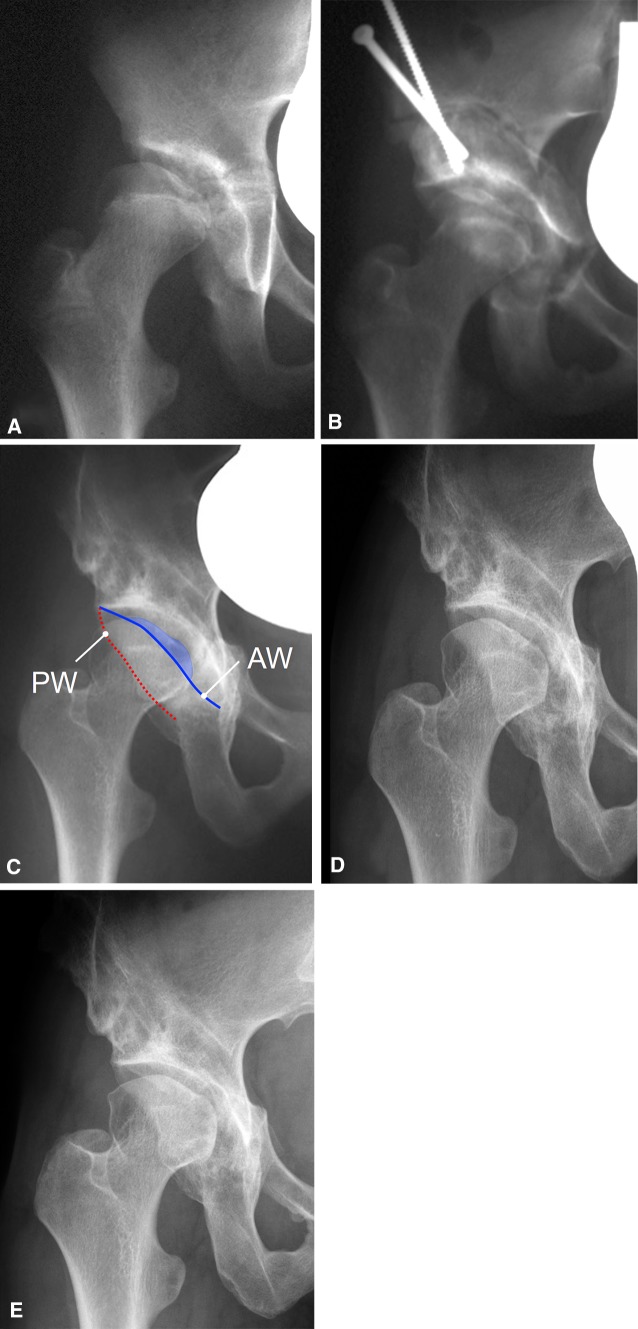
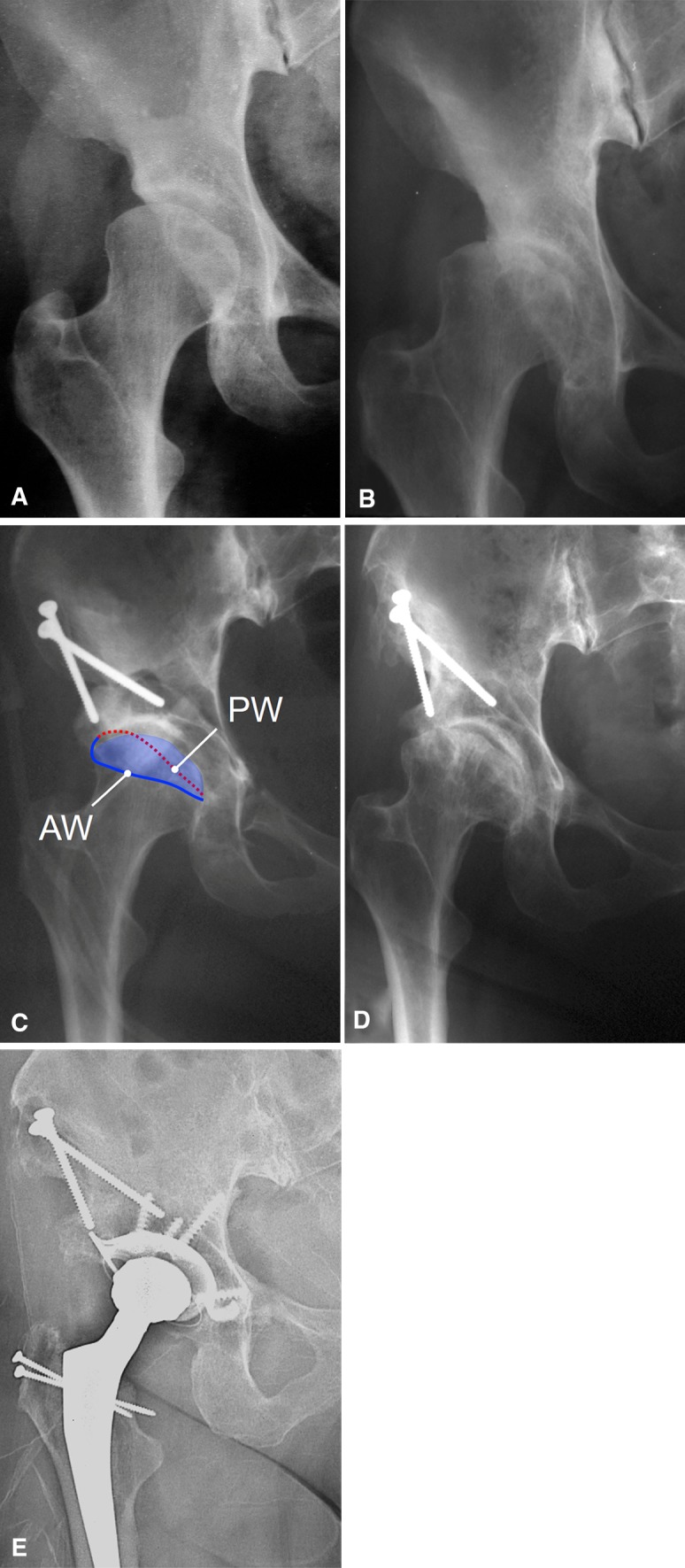
Methods: We retrospectively evaluated the first 63 patients (75 hips) who underwent PAO for hip dysplasia between 1984 and 1987. At that time, hip dysplasia was the only indication for PAO and no patients with acetabular retroversion, the second indication for a PAO performed today, were included. During that period, no other surgical treatment for hip dysplasia in patients with closed triradiate cartilage was performed. Advanced osteoarthritis (≥ Grade 2 according to Tönnis) was present preoperatively in 18 hips (24%) and 22 patients (23 hips [31%]) had previous femoral and/or acetabular surgery. Thirty-nine patients (42 hips [56%]) were converted to a THA and one patient (one hip [1%]) had hip fusion at latest followup. Two patients (three hips [4%]) died from a cause unrelated to surgery 6 and 16 years after surgery with an uneventful followup. From the remaining 21 patients (29 hips), the mean followup was 29 years (range, 27-32 years). Of those, five patients (six hips [8%]) did not return for the most recent followup and only a questionnaire was available. The cumulative survivorship of the hip according to Kaplan-Meier was calculated if any of the three endpoints, including conversion to THA, progression of osteoarthritis by at least one grade according to Tönnis, and/or a Merle d'Aubigné-Postel score < 15, occurred. Hip pain and function were assessed with Merle d'Aubigné-Postel score, Harris hip score, limp, and anterior and posterior impingement tests. Progression of radiographic osteoarthritis was assessed with Tönnis grades. A Cox regression model was used to calculate factors associated with the previously defined endpoints.
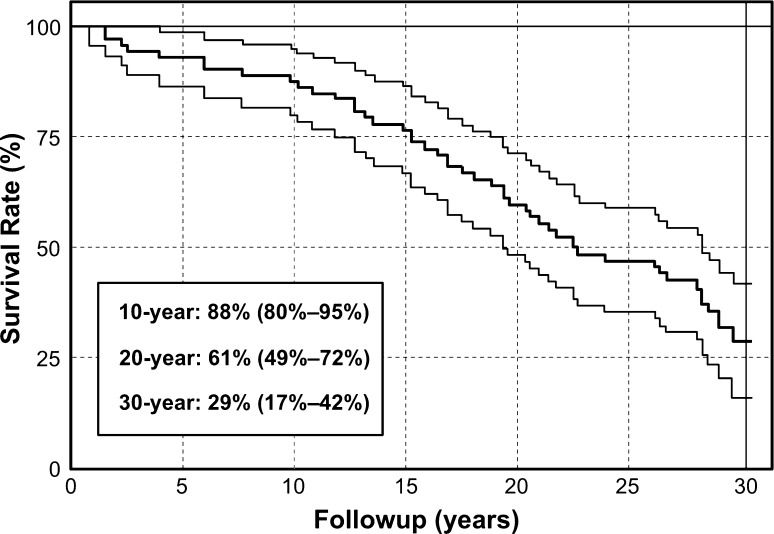
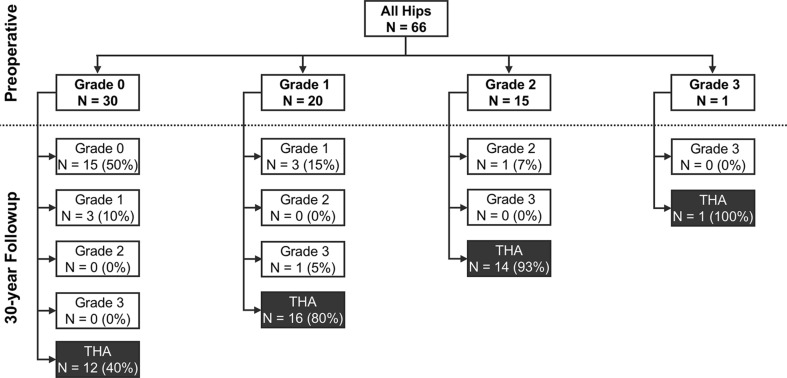
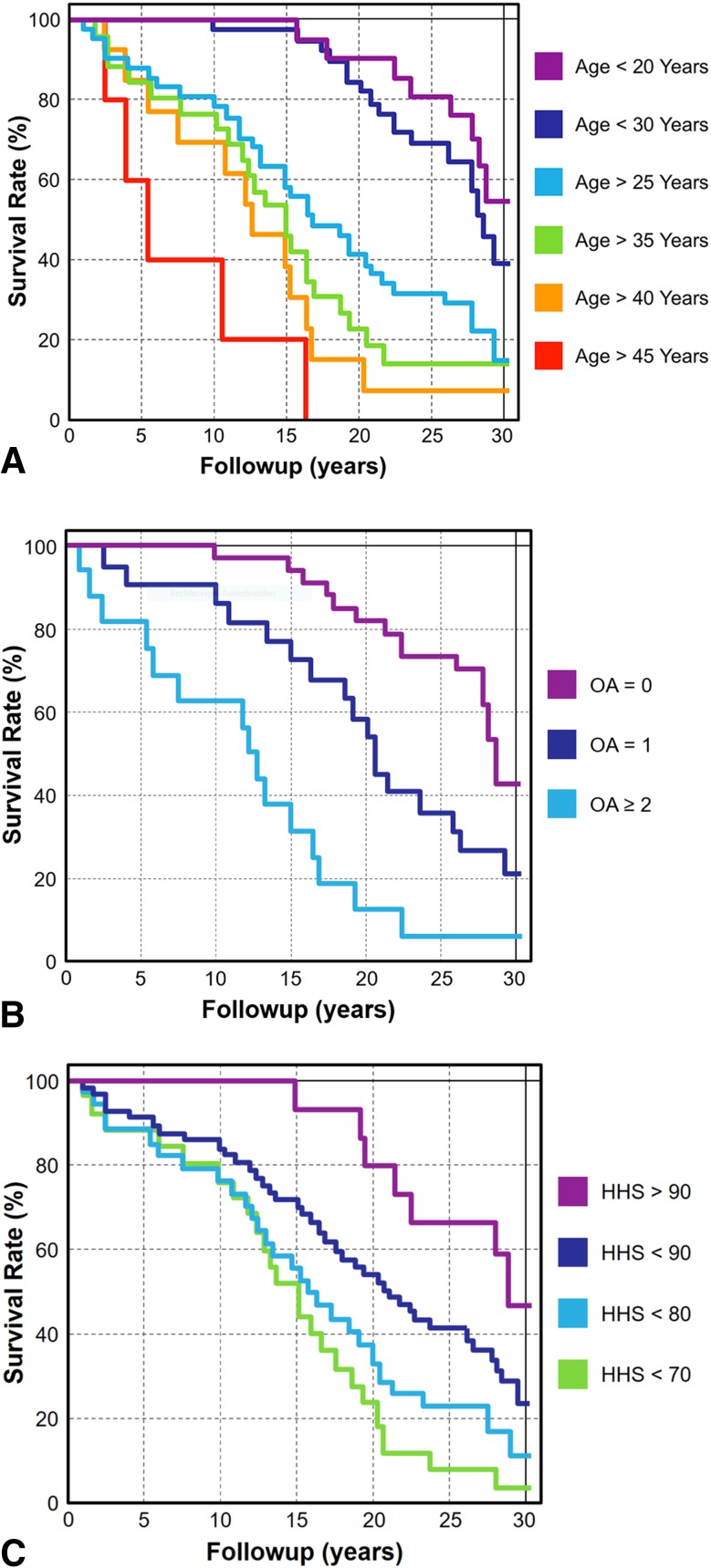
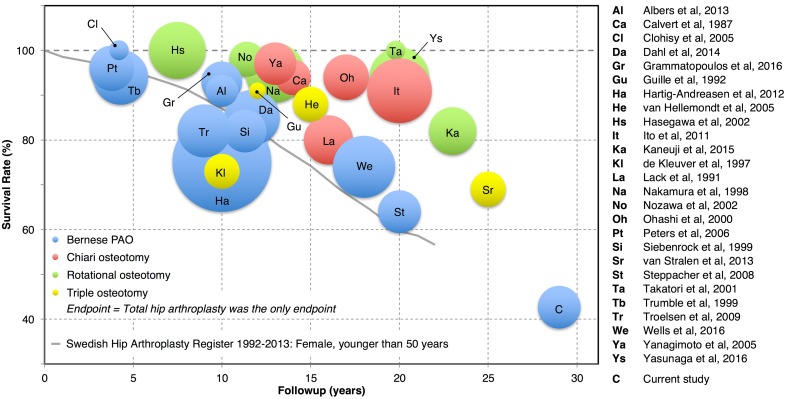
Results: The cumulative survivorship free from conversion to THA, radiographic progression of osteoarthritis, and/or Merle d'Aubigné-Postel score < 15 was 29% (95% confidence interval, 17%-42%) at 30 years. No improvement was found for either the Merle d'Aubigné-Postel (15 ± 2 versus 16 ± 2, p = 0.144) or Harris hip score (83 ± 11 versus 85 ± 17, p = 0.602). The percentage of a positive anterior impingement test (39% versus 14%, p = 0.005) decreased at 30-year followup, whereas the percentage of a positive posterior impingement test (14% versus 3%, p = 0.592) did not decrease. The percentage of positive limp decreased from preoperatively 66% to 18% at 30-year followup (p < 0.001). Mean osteoarthritis grade (Tönnis) increased from preoperatively 0.8 ± 1 (0-3) to 2.1 ± 1 (0-3) at 30-year followup (p < 0.001). Ten factors associated with poor outcome defined as THA, radiographic progression of osteoarthritis, and/or Merle d'Aubigné-Postel score < 15 were found: preoperative age > 40 years (hazard ratio [HR] 4.3 [3.7-4.9]), a preoperative Merle d'Aubigné-Postel score < 15 (HR 4.1 [3.5-4.6]), a preoperative Harris hip score < 70 (HR 5.8 [5.2-6.4]), preoperative limp (HR 1.7 [1.4-1.9]), presence of a preoperative positive anterior impingement test (HR 3.6 [3.1-4.2]), presence of a preoperative positive posterior impingement test (HR 2.5 [1.7-3.2]), a preoperative internal rotation of < 20° (HR 4.3 [3.7-4.9]), a preoperative Tönnis Grade > 1 (HR 5.7 [5.0-6.4]), a postoperative anterior coverage > 27% (HR 3.2 [2.5-3.9]), and a postoperative acetabular retroversion (HR 4.8 [3.4-6.3]).
Conclusions: Thirty years postoperatively, 29% of hips undergoing PAO for hip dysplasia can be preserved, but more than 70% will develop progressive osteoarthritis, pain, and/or undergo THA. Periacetabular osteotomy is an effective technique to treat symptomatic hip dysplasia in selected and young patients with closed triradiate cartilage. Hips with advanced joint degeneration (osteoarthritis Tönnis Grade ≥ 2) should not be treated with PAO. Postoperative anterior acetabular overcoverage or postoperative acetabular retroversion were associated with decreased joint survival.
Level of evidence: Level III, therapeutic study.
Figures
References
-
- Calvert PT, August AC, Albert JS, Kemp HB, Catterall A. The Chiari pelvic osteotomy. A review of the long-term results. J Bone Joint Surg Br. 1987;69:551–555. - PubMed
-
- Clohisy JC, Nunley RM, Curry MC, Schoenecker PL. Periacetabular osteotomy for the treatment of acetabular dysplasia associated with major aspherical femoral head deformities. J Bone Joint Surg Am. 2007;89:1417–1423. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
