

Nuclear localization of the CK2α-subunit correlates with poor prognosis in clear cell renal cell carcinoma
- PMID: 27906674
- PMCID: PMC5352082
- DOI: 10.18632/oncotarget.13693
Nuclear localization of the CK2α-subunit correlates with poor prognosis in clear cell renal cell carcinoma
Abstract
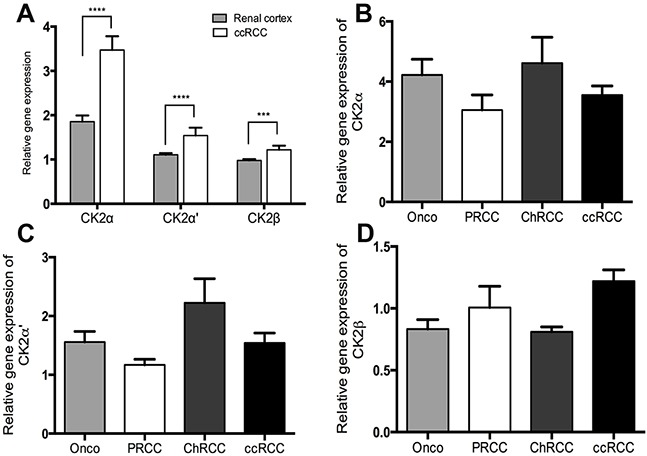
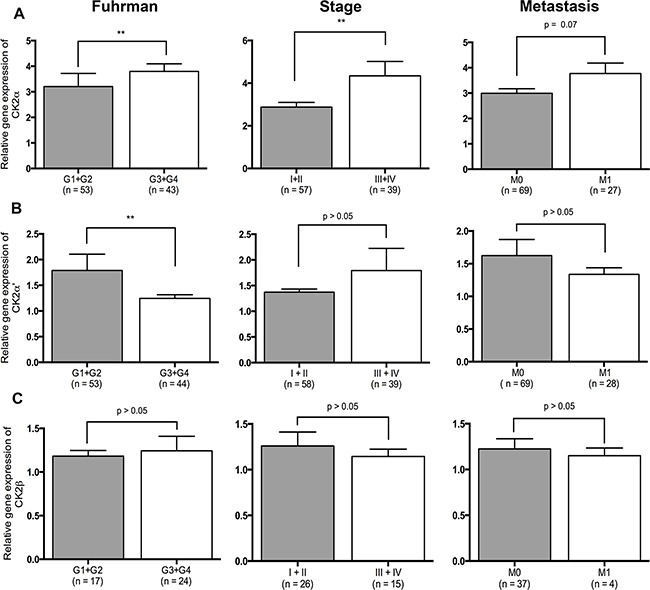
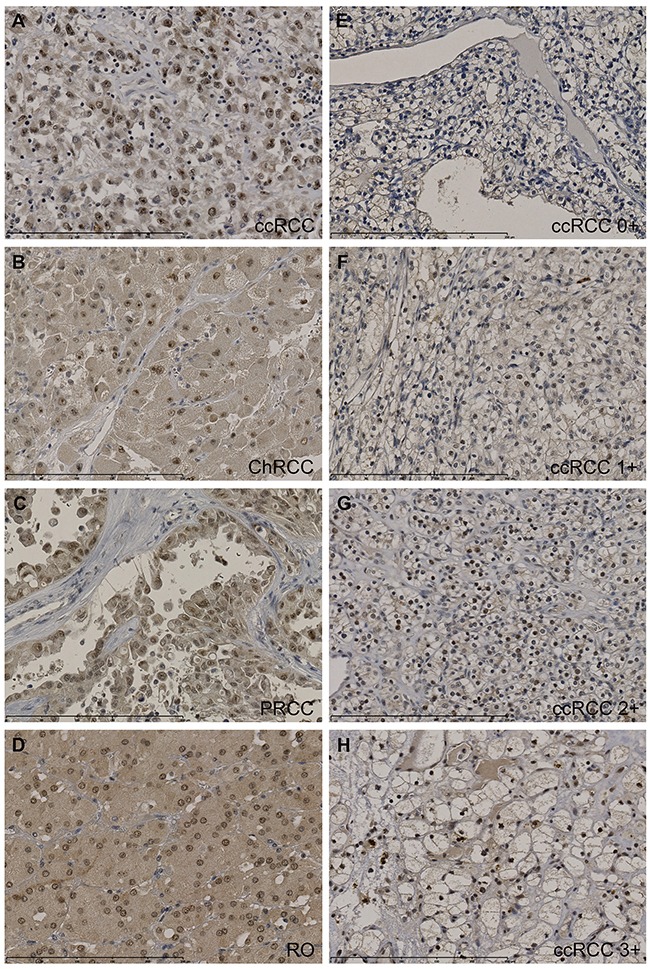
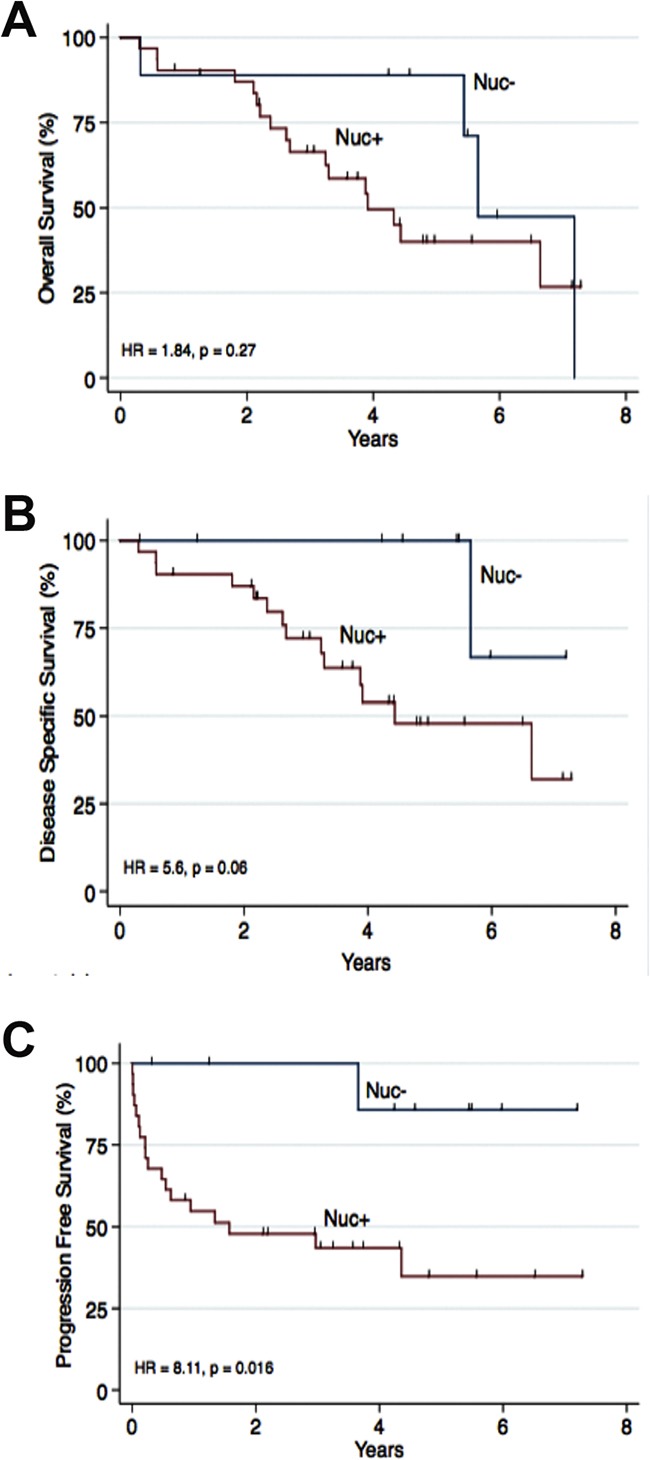
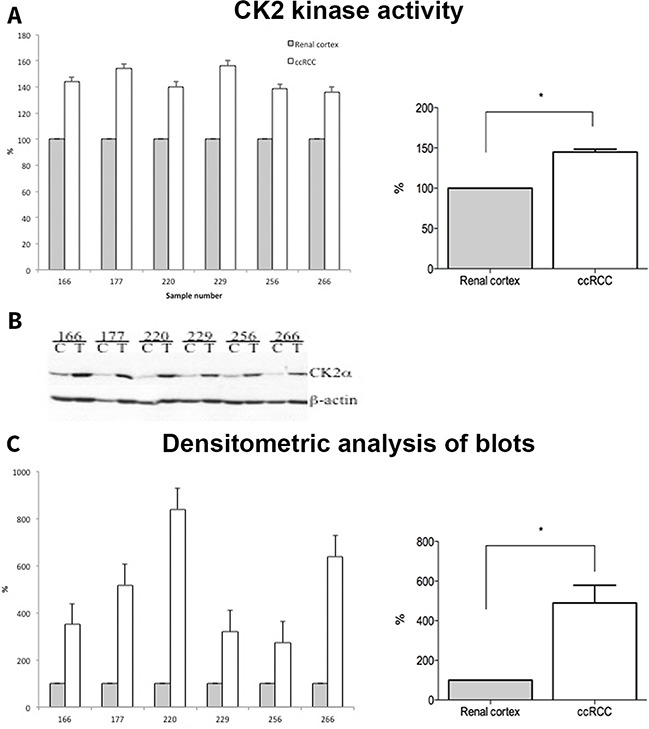
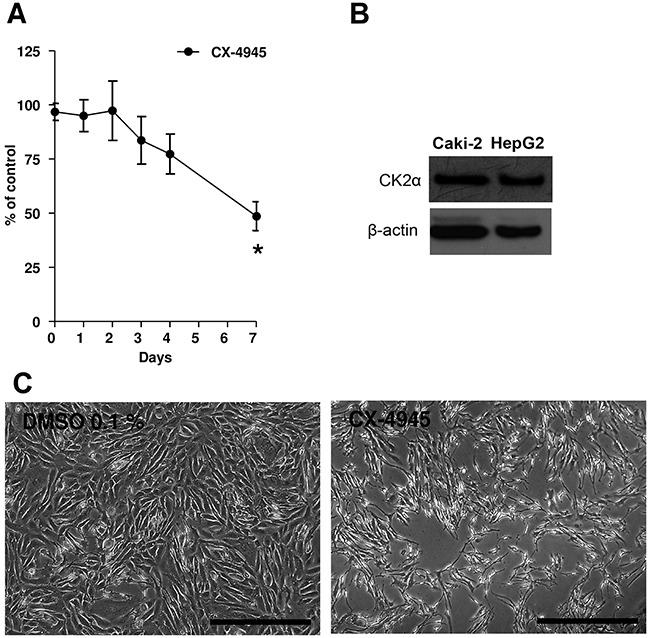
Protein kinase CK2α, one of the two catalytic isoforms of the protein kinase CK2 has been shown to contribute to tumor development, tumor proliferation and suppression of apoptosis in various malignancies. We conducted this study to investigate CK2 expression in different subtypes of Renal Cell Carcinoma (RCC) and in the benign oncocytoma. qRT-PCR, immunohistochemistry and Western blot analyses revealed that CK2α expression was significantly increased at the mRNA and protein levels in clear cell RCC (ccRCC). Also the kinase activity of CK2 was significantly increased in ccRCC compared to normal renal cortex. Nuclear protein expression of CK2α correlated in univariate analysis with poor Progression Free Survival (HR = 8.11, p = 0.016). Functional analyses (cell proliferation assay) revealed an inhibitory effect of Caki-2 cell growth following CK2 inhibition with CX-4945. Our results suggest that CK2α promotes migration and invasion of ccRCC and therefore could serve as a novel prognostic biomarker and molecular therapeutic target in this type of cancer.
Keywords: CK2 subunits; CK2-targeted therapy; CX-4945; protein kinase CK2; renal cancer.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, Rebelo M, Parkin DM, Forman D, Bray F. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. International journal of cancer. 2015;136:E359–386. - PubMed
-
- Eble JN, Sauter G., Epstein J.I., Sesterhenn I. WHO Classification of Tumours: Tumours of the Urinary System and Male Genital Organs. Lyon: IARCPress; 2004. pp. 9–88.
-
- Moch H. An overview of renal cell cancer: pathology and genetics. Semin Cancer Biol. 2013;23:3–9. - PubMed
-
- Lam JS, Leppert JT, Figlin RA, Belldegrun AS. Role of molecular markers in the diagnosis and therapy of renal cell carcinoma. Urology. 2005;66:1–9. - PubMed
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
