

Role of systematic lymphadenectomy as part of primary debulking surgery for optimally cytoreduced advanced ovarian cancer: Reappraisal in the era of radical surgery
- PMID: 27906676
- PMCID: PMC5514951
- DOI: 10.18632/oncotarget.13696
Role of systematic lymphadenectomy as part of primary debulking surgery for optimally cytoreduced advanced ovarian cancer: Reappraisal in the era of radical surgery
Abstract
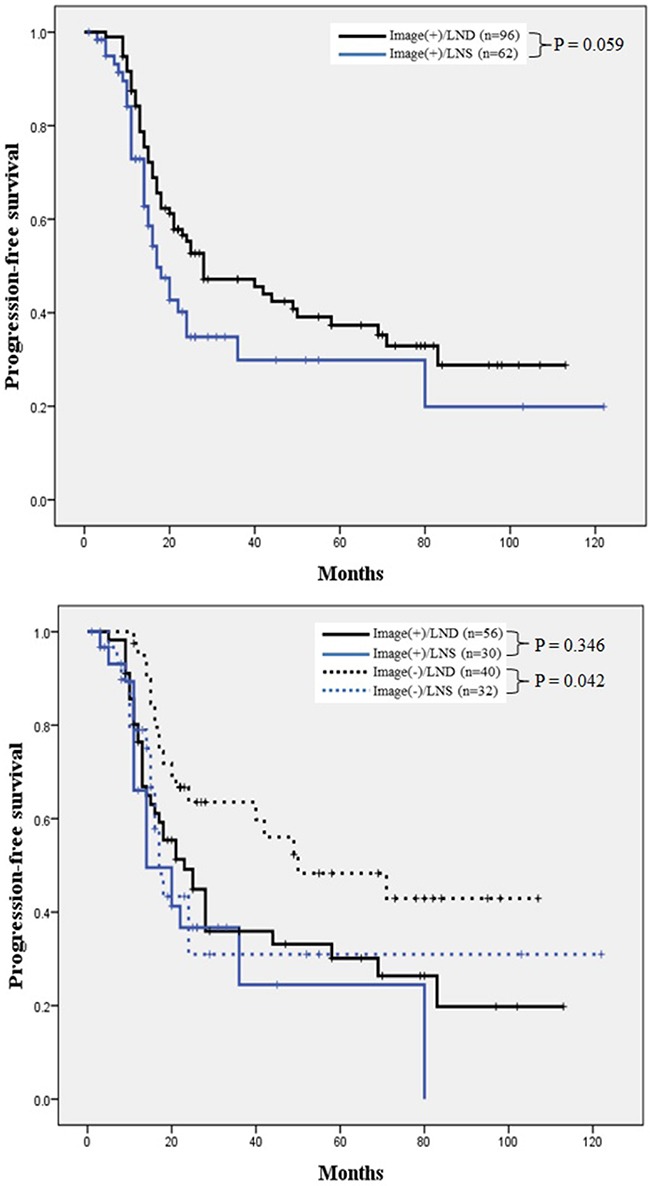
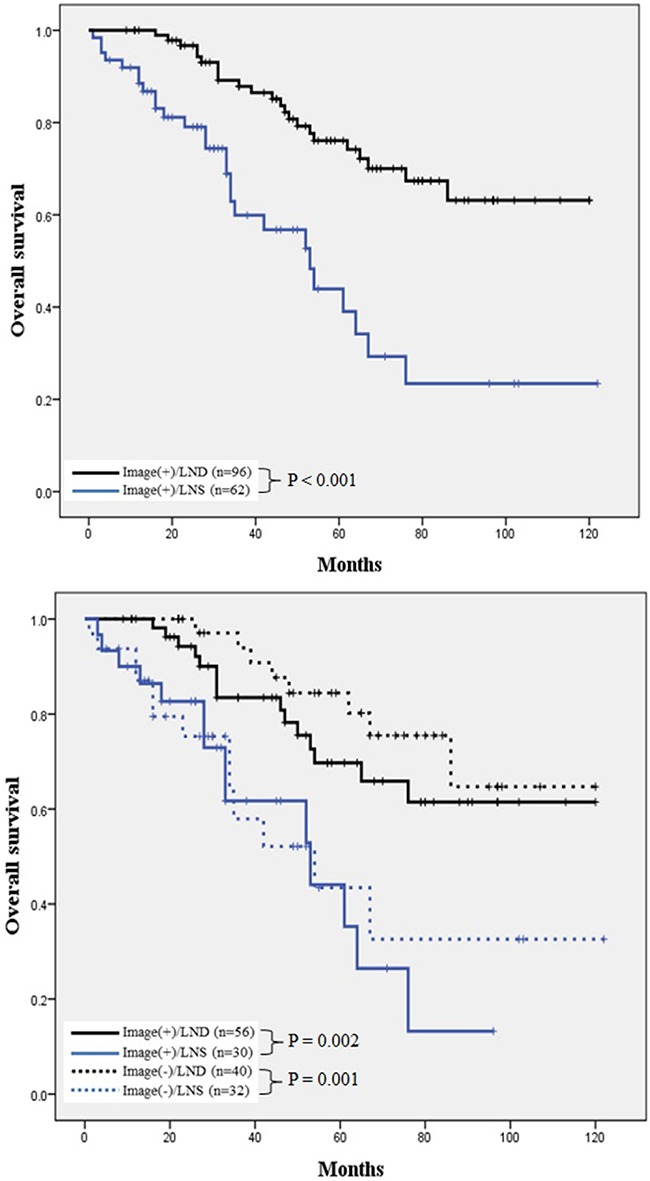
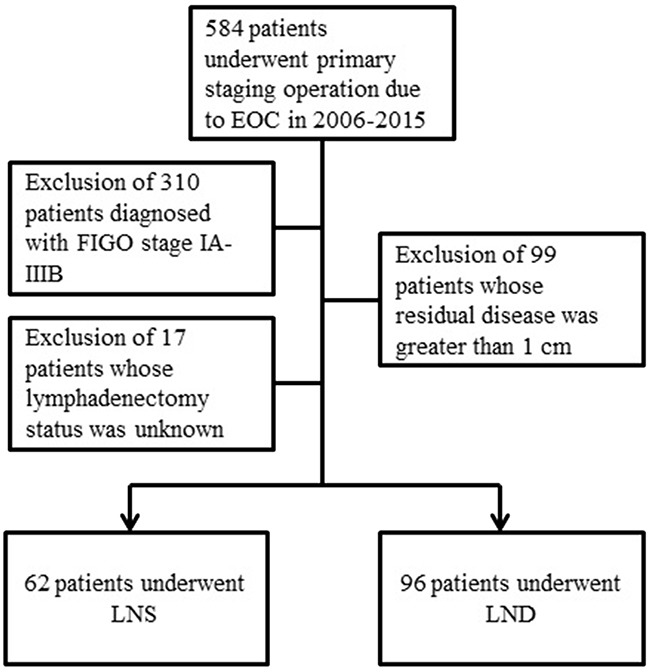
The prognostic significance of pelvic and para-aortic lymphadenectomy during primary debulking surgery for advanced-stage ovarian cancer remains unclear. This study aimed to evaluate the survival impact of lymph node dissection (LND) in patients treated with optimal cytoreduction for advanced ovarian cancer. Data from 158 consecutive patients with stage IIIC-IV disease who underwent optimal cytoreduction (<1 cm) were obtained via retrospective chart review. Patients were classified into two groups: (1) lymph node sampling (LNS), node count <20; and (2) LND, node count ≥20. Progression-free (PFS) and overall survival (OS) were analyzed using the Kaplan-Meier method. Among the included patients, 96 and 62 patients underwent LND and LNS as primary debulking surgery, respectively. There were no differences in the extent of debulking surgical procedures, including extensive upper abdominal surgery, between the groups. Patients who underwent LND had a marginally significantly improved PFS (P = 0.059) and significantly improved OS (P < 0.001) compared with those who underwent LNS. In a subgroup with negative lymphadenopathy on preoperative computed tomography scans, revealed LND correlated with a better PFS and OS (P = 0.042, 0.001, respectively). Follow-ups of subsequent recurrences observed a significantly lower nodal recurrence rate among patients who underwent LND. A multivariate analysis identified LND as an independent prognostic factor for PFS (hazard ratio [HR], 0.629; 95% confidence interval [CI], 0.400-0.989) and OS (HR, 0.250; 95% CI, 0.137-0.456). In conclusion, systematic LND might have therapeutic value and improve prognosis for patients with optimally cytoreduced advanced ovarian cancer.
Keywords: advanced epithelial ovarian cancer; lymph node dissection; lymphadenectomy; optimal cytoreductive surgery; primary debulking surgery.
Conflict of interest statement
None.
Figures
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2015. Cancer J Clin. 2015;65:5–29. - PubMed
-
- Bookman MA, Greer BE, Ozols RF. Optimal therapy of advanced ovarian cancer: carboplatin and paclitaxel vs. cisplatin and paclitaxel (GOG 158) and an update on GOG0 182-ICON5. Int J Gynecol Cancer. 2003;13:735–740. - PubMed
-
- Peiretti M, Zanagnolo V, Aletti GD, Bocciolone L, Colombo N, Landoni F, Minig L, Biffi R, Radice D, Maggioni A. Role of maximal primary cytoreductive surgery in patients with advanced epithelial ovarian and tubal cancer: Surgical and oncological outcomes. Single institution experience. Gynecol Oncol. 2010;119:259–264. - PubMed
-
- Chang SJ, Hodeib M, Chang J, Bristow RE. Survival impact of complete cytoreduction to no gross residual disease for advanced-stage ovarian cancer: a meta-analysis. Gynecol Oncol. 2013;130:493–498. - PubMed
-
- Panici PB, Maggioni A, Hacker N, Landoni F, Ackermann S, Campagnutta E, Tamussino K, Winter R, Pellegrino A, Greggi S, Angioli R, Manci N, Scambia G, et al. Systematic aortic and pelvic lymphadenectomy versus resection of bulky nodes only in optimally debulked advanced ovarian cancer: a randomized clinical trial. J Natl Cancer Inst. 2005;97:560–566. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
