

Incidence, Mortality and Positive Predictive Value of Type 1 Cardiorenal Syndrome in Acute Coronary Syndrome
- PMID: 27907067
- PMCID: PMC5132196
- DOI: 10.1371/journal.pone.0167166
Incidence, Mortality and Positive Predictive Value of Type 1 Cardiorenal Syndrome in Acute Coronary Syndrome
Abstract
Objectives: To determine whether the risk of cardiovascular mortality associated with cardiorenal syndrome subtype 1 (CRS1) in patients who were hospitalized for acute coronary syndrome (ACS) was greater than the expected risk based on the sum of its components, to estimate the predictive value of CRS1, and to determine whether the severity of CRS1 worsens the prognosis.
Methods: Follow-up study of 1912 incident cases of ACS for 1 year after discharge. Cox regression models were estimated with time to event (in-hospital death, and readmission or death during the first year after discharge) as the dependent variable.
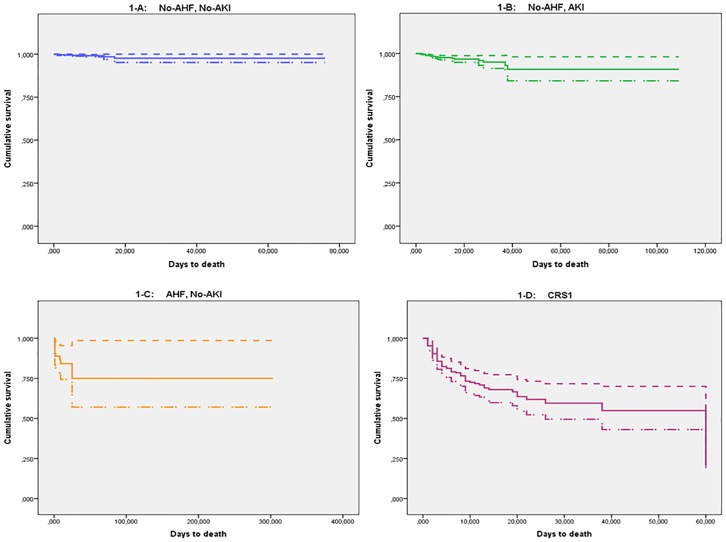
Results: The incidence of CRS1 was 9.2/1000 person-days of hospitalization (95% CI = 8.1-10.5), but these patients accounted for 56.6% (95% CI = 47.4-65.) of all mortality. The positive predictive value of CRS1 was 29.6% (95% CI = 23.9-36.0) for in-hospital death, and 51.4% (95% CI = 44.8-58.0) for readmission or death after discharge. The risk of in-hospital death from CRS1 (RR = 18.3; 95% CI = 6.3-53.2) was greater than the sum of risks associated with either acute heart failure (RR = 7.6; 95% CI = 1.8-31.8) or acute kidney injury (RR = 2.8; 95% CI = 0.9-8.8). The risk of events associated with CRS1 also increased with syndrome severity, reaching a RR of 10.6 (95% CI = 6.2-18.1) for in-hospital death at the highest severity level.
Conclusions: The effect of CRS1 on in-hospital mortality is greater than the sum of the effects associated with each of its components, and it increases with the severity of the syndrome. CRS1 accounted for more than half of all mortality, and its positive predictive value approached 30% in-hospital and 50% after discharge.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
