

Pathology of Human Coronary and Carotid Artery Atherosclerosis and Vascular Calcification in Diabetes Mellitus
- PMID: 27908890
- PMCID: PMC5269516
- DOI: 10.1161/ATVBAHA.116.306256
Pathology of Human Coronary and Carotid Artery Atherosclerosis and Vascular Calcification in Diabetes Mellitus
Abstract
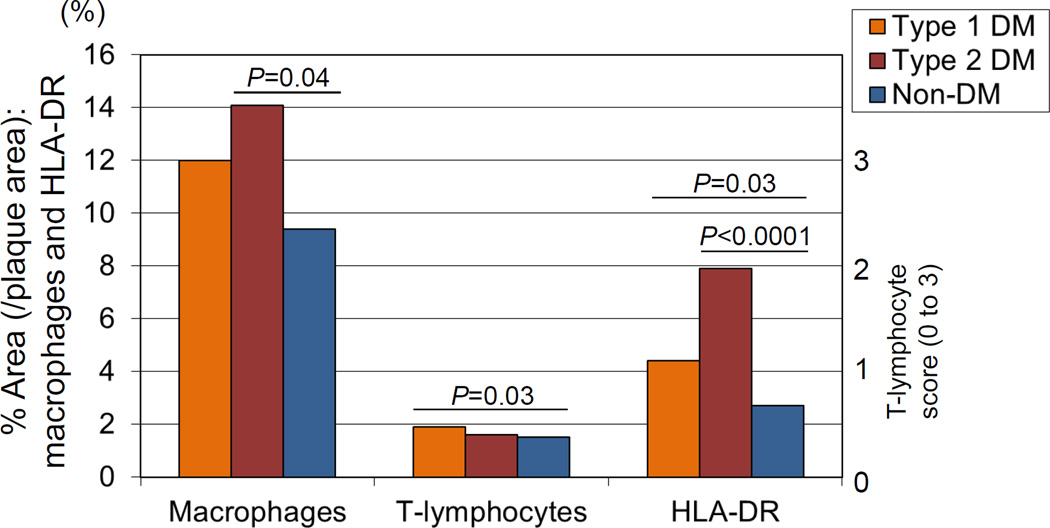
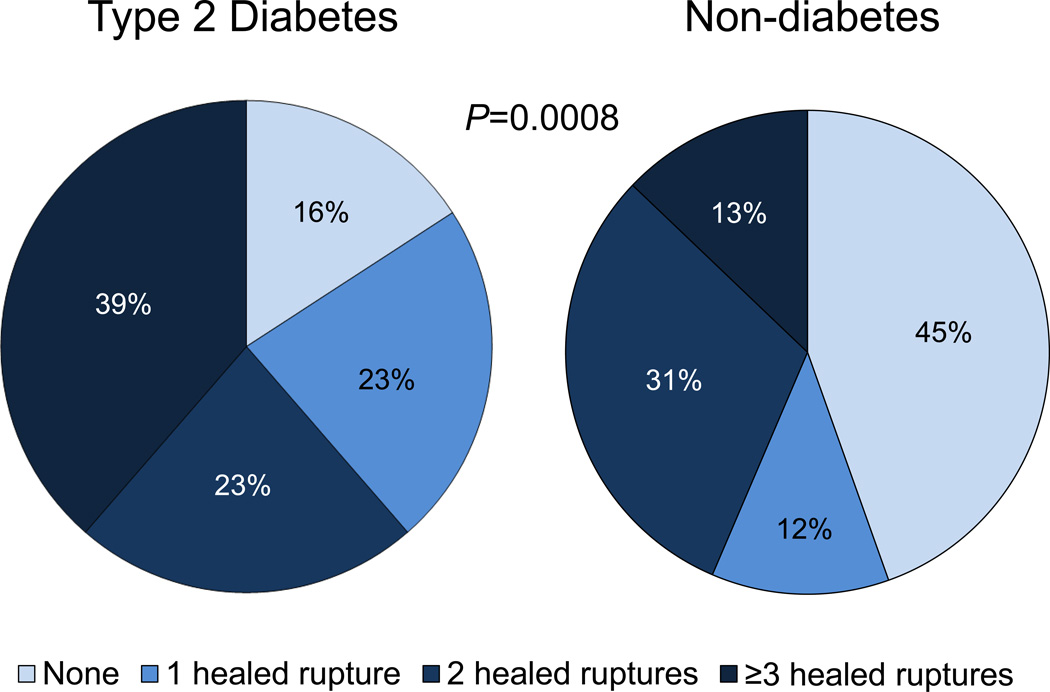
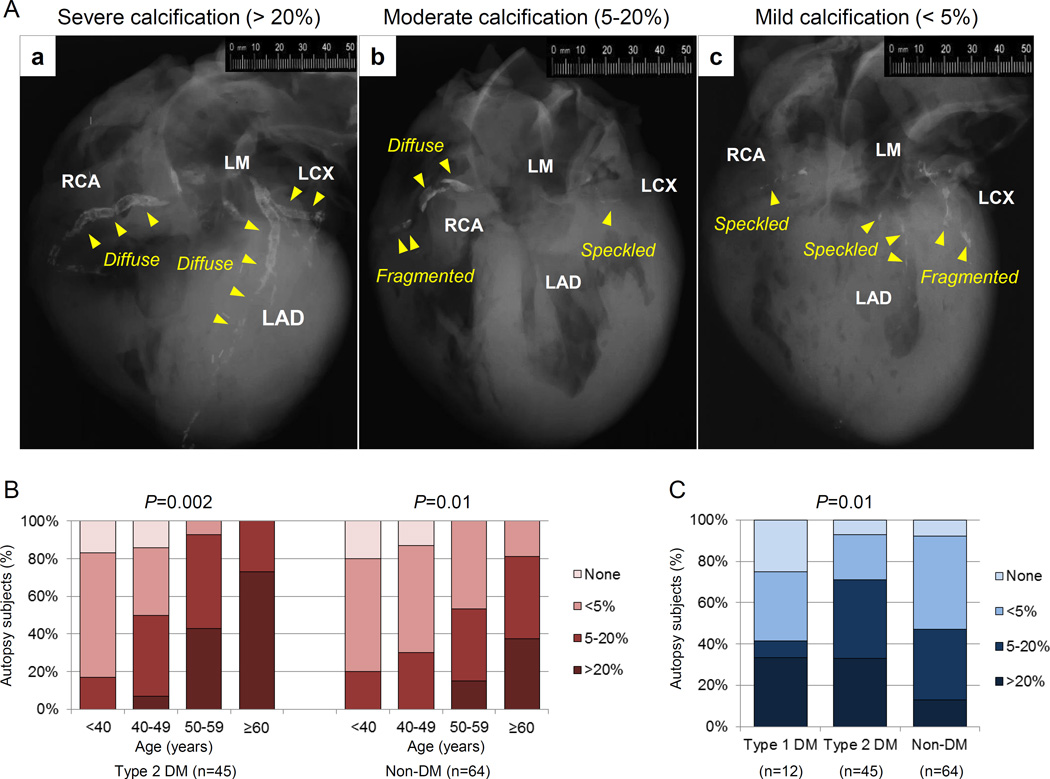
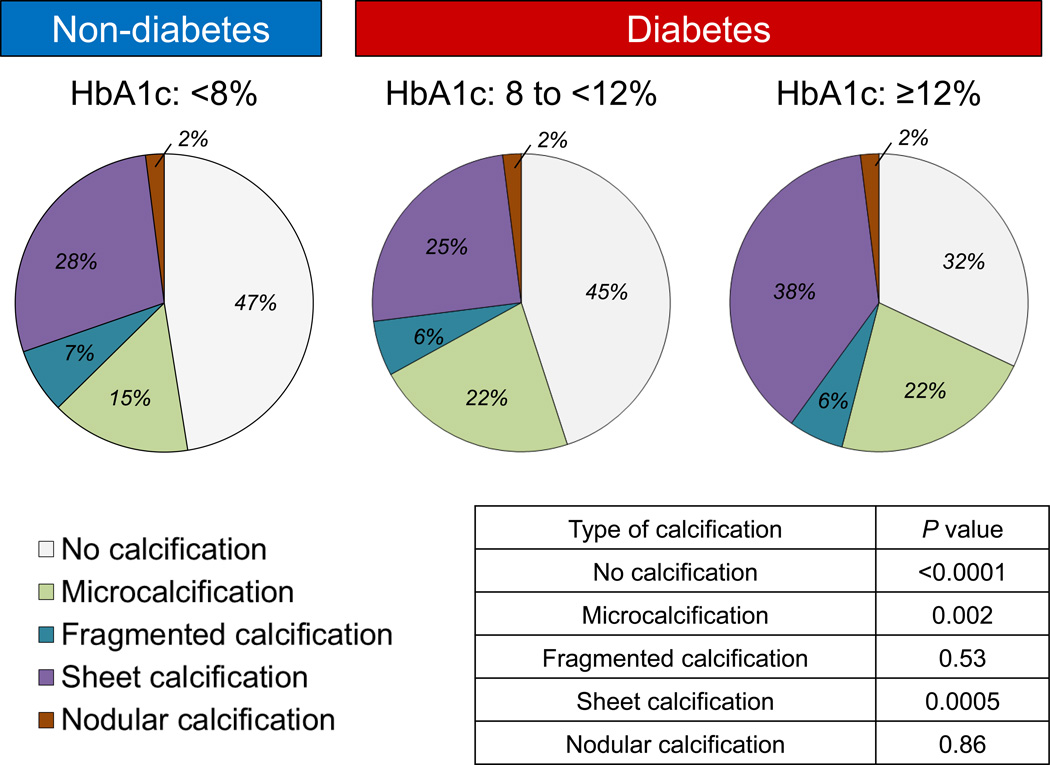
The continuing increase in the prevalence of diabetes mellitus in the general population is predicted to result in a higher incidence of cardiovascular disease. Although the mechanisms of diabetes mellitus-associated progression of atherosclerosis are not fully understood, at clinical and pathological levels, there is an appreciation of increased disease burden and higher levels of arterial calcification in these subjects. Plaques within the coronary arteries of patients with diabetes mellitus generally exhibit larger necrotic cores and significantly greater inflammation consisting mainly of macrophages and T lymphocytes relative to patients without diabetes mellitus. Moreover, there is a higher incidence of healed plaque ruptures and positive remodeling in hearts from subjects with type 1 diabetes mellitus and type 2 diabetes mellitus, suggesting a more active atherogenic process. Lesion calcification in the coronary, carotid, and other arterial beds is also more extensive. Although the role of coronary artery calcification in identifying cardiovascular disease and predicting its outcome is undeniable, our understanding of how key hormonal and physiological alterations associated with diabetes mellitus such as insulin resistance and hyperglycemia influence the process of vascular calcification continues to grow. Important drivers of atherosclerotic calcification in diabetes mellitus include oxidative stress, endothelial dysfunction, alterations in mineral metabolism, increased inflammatory cytokine production, and release of osteoprogenitor cells from the marrow into the circulation. Our review will focus on the pathophysiology of type 1 diabetes mellitus- and type 2 diabetes mellitus-associated vascular disease with particular focus on coronary and carotid atherosclerotic calcification.
Keywords: atherosclerosis; carotid arteries; coronary artery disease; death, sudden; diabetes mellitus.
© 2016 American Heart Association, Inc.
Figures
References
-
- Malmberg K, Yusuf S, Gerstein HC, Brown J, Zhao F, Hunt D, Piegas L, Calvin J, Keltai M, Budaj A. Impact of diabetes on long-term prognosis in patients with unstable angina and non-Q-wave myocardial infarction: results of the OASIS (Organization to Assess Strategies for Ischemic Syndromes) Registry. Circulation. 2000;102:1014–1019. - PubMed
-
- Mukamal KJ, Nesto RW, Cohen MC, Muller JE, Maclure M, Sherwood JB, Mittleman MA. Impact of diabetes on long-term survival after acute myocardial infarction: comparability of risk with prior myocardial infarction. Diabetes Care. 2001;24:1422–1427. - PubMed
-
- Lam DW, LeRoith D. The worldwide diabetes epidemic. Curr Opin Endocrinol Diabetes Obes. 2012;19:93–96. - PubMed
-
- Group IDFDA. Update of mortality attributable to diabetes for the IDF Diabetes Atlas: Estimates for the year 2013. Diabetes Res Clin Pract. 2015;109:461–465. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
