

Idiopathic VPC: Distribution Of FOCI And Tips Of Ablation
- PMID: 27909491
- PMCID: PMC5089466
- DOI: 10.4022/jafib.1342
Idiopathic VPC: Distribution Of FOCI And Tips Of Ablation
Abstract
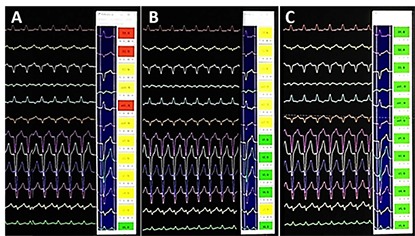
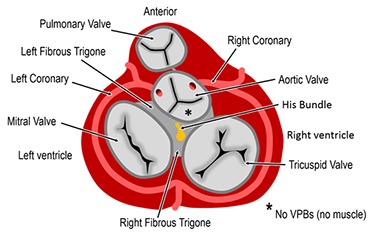
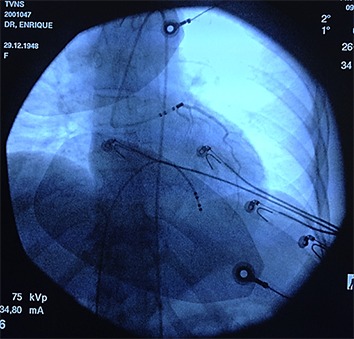
Idiopathic Ventricular Premature Contraction (VPC) is currently more routinely referred for electrophysiology evaluation. Usually it carries a good prognosis but, when symptomatic or suspected to produce ventricular dysfunction, will require treatment. Nowadays, RF ablation has great advantages over antiarrhythmic drugs. Classically the outflow tract (right or left), with the typical inferior axis with left (eventually right) bundle brunch block like ECG morphology, is considered the most frequent site of origin for idiopathic VPC, but with the widespread of EP procedures and advancement of technology making possible to map and ablate difficult locations, it is possible to see a growing and changing population referred for idiopathic VPC ablation, displaying that, almost any region of the heart may be source of this kind of arrhythmia that can be successfully treated. A well-planned procedure, with the presumed region of origin settled and employing the current technology and knowledge (tips), will have a high chance of cure.
Keywords: Ablation; Idiopathic; Outflow tract; Ventricular Premature Contraction.
Figures
References
-
- Dukes Jonathan W, Dewland Thomas A, Vittinghoff Eric, Mandyam Mala C, Heckbert Susan R, Siscovick David S, Stein Phyllis K, Psaty Bruce M, Sotoodehnia Nona, Gottdiener John S, Marcus Gregory M. Ventricular Ectopy as a Predictor of Heart Failure and Death. J. Am. Coll. Cardiol. 2015 Jul 14;66 (2):101–9. - PMC - PubMed
-
- Hasdemir Can, Ulucan Cem, Yavuzgil Oguz, Yuksel Alper, Kartal Yildirim, Simsek Evrim, Musayev Oktay, Kayikcioglu Meral, Payzin Serdar, Kultursay Hakan, Aydin Mehmet, Can Levent H. Tachycardia-induced cardiomyopathy in patients with idiopathic ventricular arrhythmias: the incidence, clinical and electrophysiologic characteristics, and the predictors. J. Cardiovasc. Electrophysiol. 2011 Jun;22 (6):663–8. - PubMed
-
- Penela Diego, De Riva Marta, Herczku Csaba, Catto Valentina, Pala Salvatore, Fernández-Armenta Juan, Acosta Juan, Cipolletta Laura, Andreu David, Borras Roger, Rios Jose, Mont Lluis, Brugada Josep, Carbucicchio Corrado, Zeppenfeld Katja, Berruezo Antonio. An easy-to-use, operator-independent, clinical model to predict the left vs. right ventricular outflow tract origin of ventricular arrhythmias. Europace. 2015 Jul;17 (7):1122–8. - PubMed
-
- Latchamsetty R, Yokokawa M, Morady F. Multicenter outcomes for catheter ablation of idiopathic premature ventricular complexes. J Am Coll Cardiol EP. 2015;1:116–23.
Publication types
LinkOut - more resources
Full Text Sources