

Long-Term Evolution of Patients Treated for Paroxysmal Atrial Fibrillation with First and Second Generation Cryoballoon Catheter Ablation with a Prospective Protocol Guided by Complete Bidirectional Left Atrium-Pulmonary Veins Disconnection after Adenosine as Main Target end Point to achieved. Seven Years Follow-up of Patients with a rough estimation profile of Low ALARMEc Score. A Single Center Report
- PMID: 27909504
- PMCID: PMC5089479
- DOI: 10.4022/jafib.1400
Long-Term Evolution of Patients Treated for Paroxysmal Atrial Fibrillation with First and Second Generation Cryoballoon Catheter Ablation with a Prospective Protocol Guided by Complete Bidirectional Left Atrium-Pulmonary Veins Disconnection after Adenosine as Main Target end Point to achieved. Seven Years Follow-up of Patients with a rough estimation profile of Low ALARMEc Score. A Single Center Report
Abstract
Introduction: Cryoballoon ablation (CB) has proven effective for treating patients with paroxysmal atrial fibrillation (PAF). We analyzed our seven year follow-up of patients, treated for PAF with first (CB1) and second generation (CB2), with demonstration of LA-PV disconnection with bidirectional block (BB) after adenosine (AD).
Methods: Since November 2008 to May 2015, 128 patients, 97 male (58±7 years), without heart disease, highly symptomatic, refractory to antiarrhythmic drugs (AAD) were treated, and follow-up (1411 ±727 days). Left atrial size: 37±6 mm.
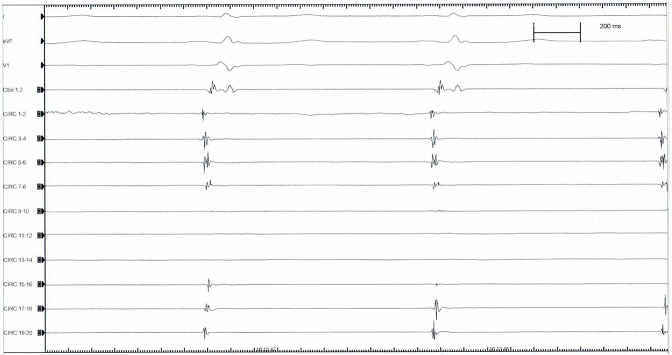
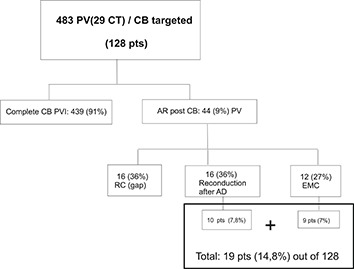
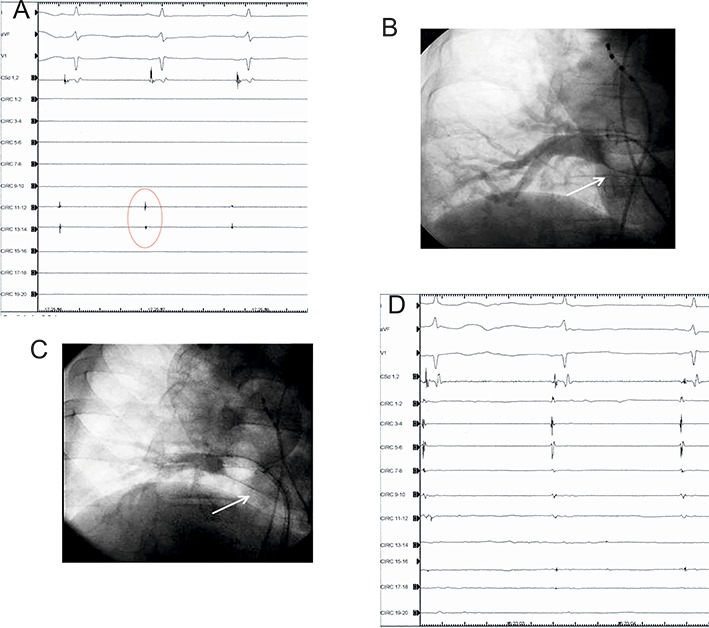
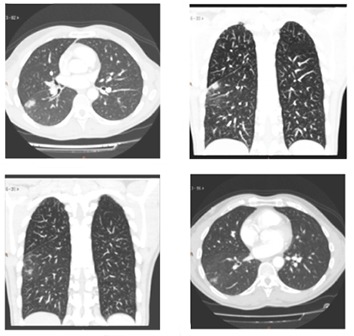
Results: A total of 439 PV were successfully isolated (91.9%). Acute reconduction: 44 PV (9%): 16 after CB; 16 unmasked by AD; 12 extrapulmonary muscular connections (EMC). Main complication was phrenic nerve palsy (PNP): 9 (7 %). On follow-up, 114 patients (89%) remain asymptomatic in sinus rhythm (SR), free of medication. Fourteen patients (11%) had arrhythmia recurrence: 12 male (52±8 years). Early recurrences occurred in 9 male. Late recurrences presented 3 male at 24, 27 and 60 months, and 2 female at 7 and 40 months respectively. All recurrence patients were Redo, and remain in SR without medication during follow-up.
Conclusions: CB alone is very effective and safe for the definitive treatment of patients suffering PAF with 72.6% success rate, increasing up to 89.1% when this protocol is applied in a single procedure. After Redo, all population group (100%), remain in sinus rhythm, freedom of arrhythmia, without AAD, in this very long term follow-up. Checking for BB, AD protocol, and ruling out EMC allowed-us to identified 14.8% of patients with underlying substrate for potential arrhythmia recurrence. CB2 applications entail a highest risk of PNP. Patients with a rough estimated profile of low ALARMEc score (≤ 1) have an excellent long term outcome, being this series the largest follow-up described so far, for patients treated for PAF with CB.
Keywords: Ablation; Cryoballoon; Paroxysmal Atrial Fibrillation.
Figures










Similar articles
-
First And Second-Generation Cryoballoon Ablation Efficacy Restoring And Maintaining Sinus Rhythm In Patients Electrically Selected And Treated For Long-Standing Persistent Atrial Fibrillation After Acute Complete Electrical Disconnection Of Pulmonary Veins From The Left Atrium Demonstrated.J Atr Fibrillation. 2016 Apr 30;8(6):1399. doi: 10.4022/jafib.1399. eCollection 2016 Apr-May. J Atr Fibrillation. 2016. PMID: 27909503 Free PMC article.
-
Two-year clinical outcome after a single cryoballoon ablation procedure: A comparison of first- and second-generation cryoballoons.Arch Cardiovasc Dis. 2017 Oct;110(10):543-549. doi: 10.1016/j.acvd.2017.01.015. Epub 2017 Sep 25. Arch Cardiovasc Dis. 2017. PMID: 28958871
-
One-year follow-up after single procedure Cryoballoon ablation: a comparison between the first and second generation balloon.J Cardiovasc Electrophysiol. 2014 Aug;25(8):834-839. doi: 10.1111/jce.12409. Epub 2014 Apr 9. J Cardiovasc Electrophysiol. 2014. PMID: 24641307
-
Second generation cryoballoon ablation for persistent atrial fibrillation: an updated meta-analysis.Clin Res Cardiol. 2018 Feb;107(2):182-192. doi: 10.1007/s00392-017-1171-5. Epub 2017 Oct 26. Clin Res Cardiol. 2018. PMID: 29075979 Review.
-
Cryoballoon versus Radiofrequency Catheter Ablation in Atrial Fibrillation: A Meta-Analysis.J Cardiovasc Electrophysiol. 2016 Oct;27(10):1151-1159. doi: 10.1111/jce.13047. Epub 2016 Aug 16. J Cardiovasc Electrophysiol. 2016. PMID: 27422848 Review.
Cited by
-
Clinical scores used for the prediction of negative events in patients undergoing catheter ablation for atrial fibrillation.Clin Cardiol. 2019 Feb;42(2):320-329. doi: 10.1002/clc.23139. Epub 2019 Jan 14. Clin Cardiol. 2019. PMID: 30578568 Free PMC article. Review.
References
-
- Haïssaguerre M, Jaïs P, Shah D C, Takahashi A, Hocini M, Quiniou G, Garrigue S, Le Mouroux A, Le Métayer P, Clémenty J. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N. Engl. J. Med. 1998 Sep 3;339 (10):659–66. - PubMed
-
- Jaïs P, Haïssaguerre M, Shah D C, Chouairi S, Gencel L, Hocini M, Clémenty J. A focal source of atrial fibrillation treated by discrete radiofrequency ablation. Circulation. 1997 Feb 4;95 (3):572–6. - PubMed
-
- Haïssaguerre M, Shah D C, Jaïs P, Hocini M, Yamane T, Deisenhofer I, Chauvin M, Garrigue S, Clémenty J. Electrophysiological breakthroughs from the left atrium to the pulmonary veins. Circulation. 2000 Nov 14;102 (20):2463–5. - PubMed
-
- Oral Hakan, Knight Bradley P, Tada Hiroshi, Ozaydin Mehmet, Chugh Aman, Hassan Sohail, Scharf Christoph, Lai Steve W K, Greenstein Radmira, Pelosi Frank, Strickberger S Adam, Morady Fred. Pulmonary vein isolation for paroxysmal and persistent atrial fibrillation. Circulation. 2002 Mar 5;105 (9):1077–81. - PubMed
-
- Van Belle Yves, Janse Petter, Rivero-Ayerza Maximo J, Thornton Andrew S, Jessurun Emile R, Theuns Dominic, Jordaens Luc. Pulmonary vein isolation using an occluding cryoballoon for circumferential ablation: feasibility, complications, and short-term outcome. Eur. Heart J. 2007 Sep;28 (18):2231–7. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous