

Reliability of the Planned Pedicle Screw Trajectory versus the Actual Pedicle Screw Trajectory using Intra-operative 3D CT and Image Guidance
- PMID: 27909659
- PMCID: PMC5130325
- DOI: 10.14444/3038
Reliability of the Planned Pedicle Screw Trajectory versus the Actual Pedicle Screw Trajectory using Intra-operative 3D CT and Image Guidance
Abstract
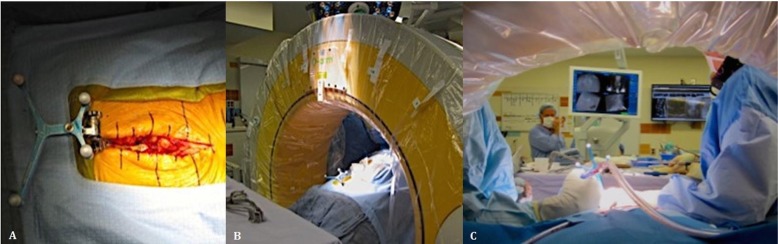
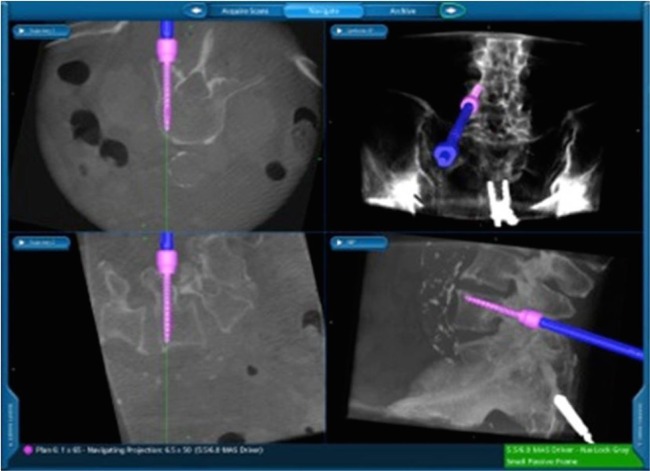
Background: Technological advances, including navigation, have been made to improve safety and accuracy of pedicle screw fixation. We evaluated the accuracy of the virtual screw placement (Stealth projection) compared to actual screw placement (intra-operative O-Arm) and examined for differences based on the distance from the reference frame.
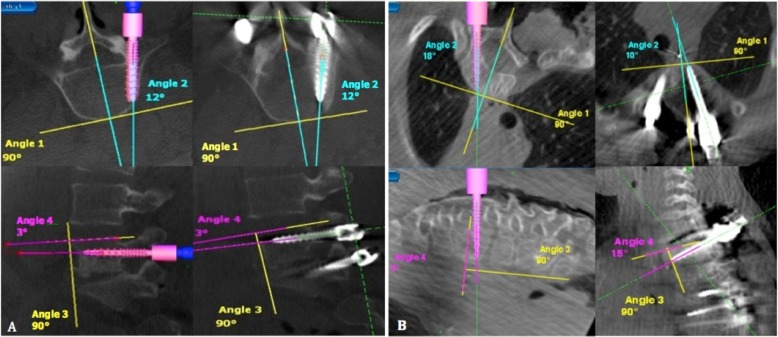
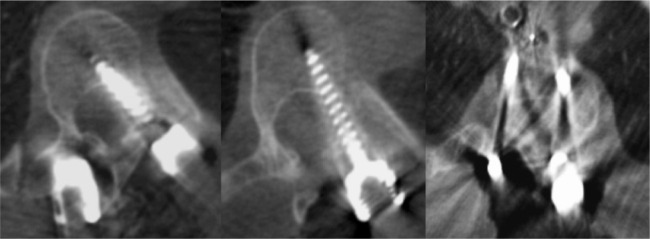
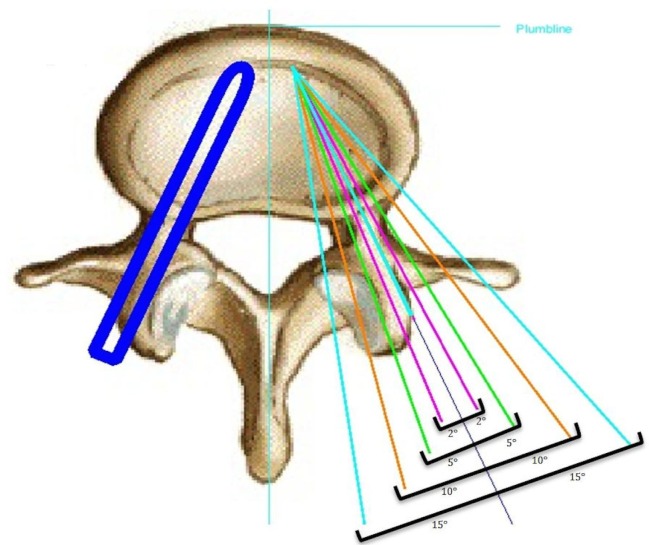
Methods: A retrospective evaluation of prospectively collected data was conducted from January 2013 to September 2013. We evaluated thoracic and lumbosacral pedicle screws placed using intraoperative O-arm and Stealth navigation by obtaining virtual screw projections and intraoperative O-arm images after screw placement. The screw trajectory angle to the midsagittal line and superior endplate was compared in the axial and sagittal views, respectively. Percent error and paired t-test statistics were then performed.
Results: Thirty-one patients with 240 pedicle screws were analyzed. The mean angular difference between the virtual and actual image in all screws was 2.17° ± 2.20° on axial images and 2.16° ± 2.24° on sagittal images. There was excellent agreement between actual and virtual pedicle screw trajectories in the axial and sagittal plane with ICC = 0.99 (95%CI: 0.992-0.995) (p<0.001) and ICC= 0.81 (95%CI: 0.759-0.855) (p<0.001) respectively. When comparing thoracic and lumbar screws, there was a significant difference in the sagittal angulation between the two distributions. No statistical differences were found distance from the reference frame.
Conclusion: The virtual projection view is clinically accurate compared to the actual placement on intra-operative CT in both the axial and sagittal views. There is slight imprecision (~2°) in the axial and sagittal planes and a minor difference in the sagittal thoracic and lumbar angulation, although these did not affect clinical outcomes. In general, we find that pedicle screw placement using intraoperative cone beam CT and navigation to be accurate and reliable, and as such have made it a routine part of our spine practice. This study was approved by the University of Minnesota IRB (#1303E30544).
Keywords: accuracy; navigation; pedicle screws.
Figures

References
-
- KING D. Internal fixation for lumbosacral fusion. J Bone Joint Surg Am. 1948;30A(3):560–565. - PubMed
-
- BOUCHER HH. A method of spinal fusion. J Bone Joint Surg Br. 1959;41-B(2):248–259. - PubMed
-
- Roy-Camille R, Saillant G, Berteaux D, Salgado V. Osteosynthesis of thoraco-lumbar spine fractures with metal plates screwed through the vertebral pedicles. Reconstr Surg Traumatol. 1976;15:2–16. - PubMed
-
- Ledonio CG, Polly DW, Jr, Vitale MG, Wang Q, Richards BS. Pediatric pedicle screws: Comparative effectiveness and safety: A systematic literature review from the scoliosis research society and the pediatric orthopaedic society of north america task force. J Bone Joint Surg Am. 2011;93(13):1227–1234. doi: 10.2106/JBJS.J.00678. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources