

Tibial hemimelia: new classification and reconstructive options
- PMID: 27909860
- PMCID: PMC5145835
- DOI: 10.1007/s11832-016-0785-x
Tibial hemimelia: new classification and reconstructive options
Abstract
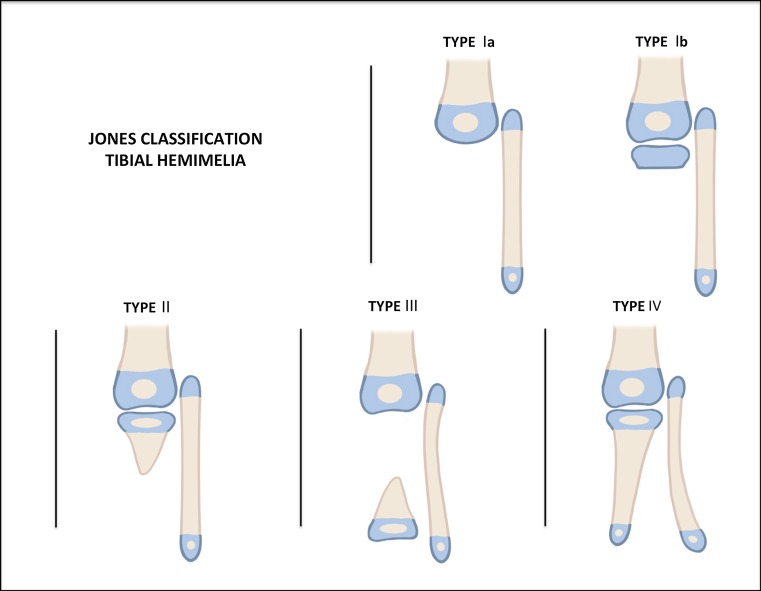
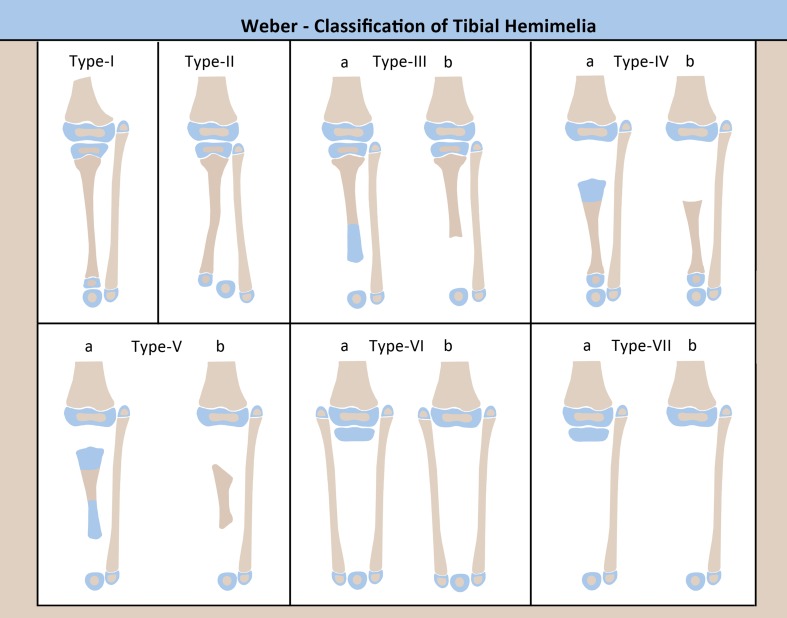
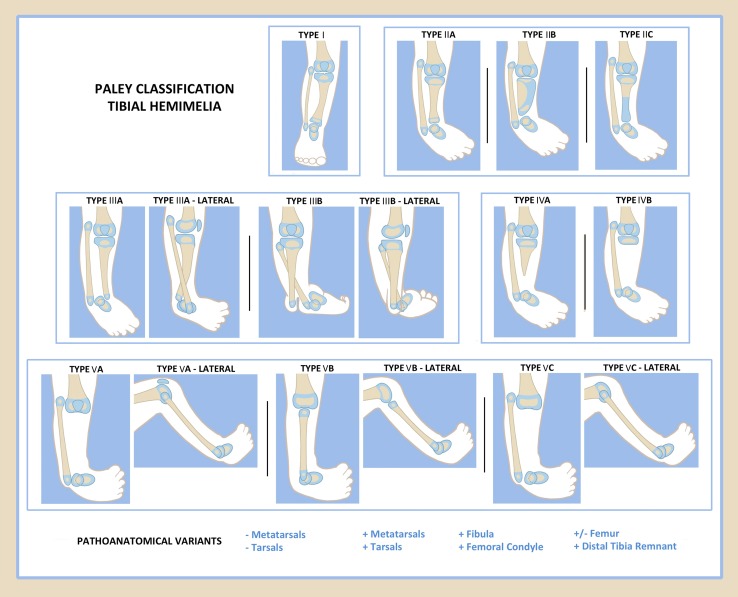
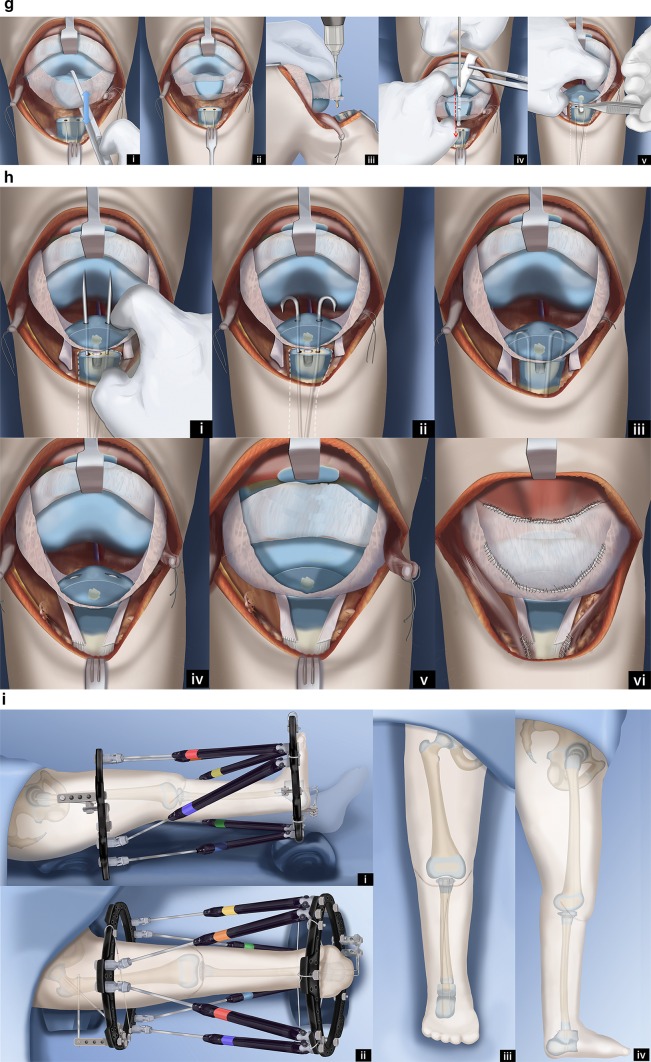
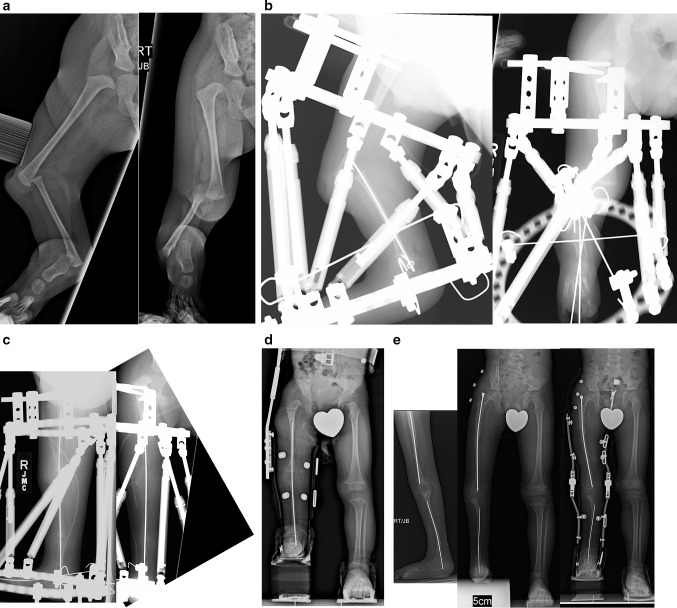
Tibial hemimelia is a rare congenital lower limb deficiency presenting with a wide spectrum of associated congenital anomalies, deficiencies and duplications. Reconstructive options have been limited, and the gold standard for treatment has remained amputation with prosthetic fitting. There is now a better understanding of the genetics, etiology and pathoanatomy of tibial hemimelia. Armed with this knowledge, I present here a new classification to guide treatment and prognosis and then discuss new treatment strategies and techniques for limb reconstruction based on this new classification scheme.
Keywords: Brown centralization of fibula; Clubfoot; Paley classification; Tibial aplasia; Tibial hemimelia; Weber patelloplasty.
Figures


Similar articles
-
Systematic radiographic evaluation of tibial hemimelia with orthopedic implications.Pediatr Radiol. 2017 Apr;47(4):473-483. doi: 10.1007/s00247-016-3730-8. Epub 2017 Jan 3. Pediatr Radiol. 2017. PMID: 28050636 Review.
-
Usual Presentation Has Odds: Unilateral Tibial Hemimelia in One of Dizygotic Twins.Cureus. 2021 Jan 21;13(1):e12834. doi: 10.7759/cureus.12834. Cureus. 2021. PMID: 33633877 Free PMC article.
-
Deformity Reconstruction Surgery for Tibial Hemimelia.Children (Basel). 2021 May 31;8(6):461. doi: 10.3390/children8060461. Children (Basel). 2021. PMID: 34072809 Free PMC article. Review.
-
[Clubfoot associated with tibial and fibular hemimelia].Z Orthop Unfall. 2012 Oct;150(5):525-32. doi: 10.1055/s-0032-1314997. Epub 2012 Oct 17. Z Orthop Unfall. 2012. PMID: 23076751 German.
-
Amputation Versus Limb Reconstruction for Fibula Hemimelia: A Meta-analysis.J Pediatr Orthop. 2020 Sep;40(8):425-430. doi: 10.1097/BPO.0000000000001510. J Pediatr Orthop. 2020. PMID: 31972725
Cited by
-
Prenatal diagnosis of tibial hemimelia type I and omphalocele, a rare entity and postnatal correlation.BJR Case Rep. 2020 Sep 4;7(1):20200002. doi: 10.1259/bjrcr.20200002. eCollection 2021 Feb 1. BJR Case Rep. 2020. PMID: 33614110 Free PMC article.
-
Systematic radiographic evaluation of tibial hemimelia with orthopedic implications.Pediatr Radiol. 2017 Apr;47(4):473-483. doi: 10.1007/s00247-016-3730-8. Epub 2017 Jan 3. Pediatr Radiol. 2017. PMID: 28050636 Review.
-
Usual Presentation Has Odds: Unilateral Tibial Hemimelia in One of Dizygotic Twins.Cureus. 2021 Jan 21;13(1):e12834. doi: 10.7759/cureus.12834. Cureus. 2021. PMID: 33633877 Free PMC article.
-
The need for state-of-the-art orthopedic surgical technology in low- to middle income countries : The case of distraction epiphyseolysis for limb lengthening in children with fibular hemimelia in Uzbekistan.Arch Orthop Trauma Surg. 2024 Sep;144(9):4375-4383. doi: 10.1007/s00402-024-05537-6. Epub 2024 Sep 26. Arch Orthop Trauma Surg. 2024. PMID: 39327267
-
Bilateral Calcaneus Transfers for the Treatment of Congenital Tibial Deficiencies: A Novel Surgical Technique and Case Report.J Am Acad Orthop Surg Glob Res Rev. 2022 Dec 5;6(12):e22.00070. doi: 10.5435/JAAOSGlobal-D-22-00070. eCollection 2022 Dec 1. J Am Acad Orthop Surg Glob Res Rev. 2022. PMID: 36732306 Free PMC article.
References
-
- Aitkin GT, Bose K, Brown FW et al (1998) Tibial hemimelia. In: Canale ST (ed) Campbell’s operative orthopaedics. Mosby-Year Book, St Louis, pp 937–938, 967–972, 1001–1003
-
- Jose RM, Kamath AK, Vijayaraghavan S, Varghese S, Nair SR, Nandakumar UR. Tibial hemimelia with ‘mirror foot’. Eur J Plast Surg. 2004;27(1):39–41. doi: 10.1007/s00238-004-0609-y. - DOI
-
- Yetkin H, Cila E, Bilgin Guzel V, Kanatli U. Femoral bifurcation associated with tibial hemimelia. Orthopedics. 2001;24:389. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
