

Can We Estimate Short- and Intermediate-term Survival in Patients Undergoing Surgery for Metastatic Bone Disease?
- PMID: 27909972
- PMCID: PMC5339146
- DOI: 10.1007/s11999-016-5187-3
Can We Estimate Short- and Intermediate-term Survival in Patients Undergoing Surgery for Metastatic Bone Disease?
Abstract
Background: Objective means of estimating survival can be used to guide surgical decision-making and to risk-stratify patients for clinical trials. Although a free, online tool ( www.pathfx.org ) can estimate 3- and 12-month survival, recent work, including a survey of the Musculoskeletal Tumor Society, indicated that estimates at 1 and 6 months after surgery also would be helpful. Longer estimates help justify the need for more durable and expensive reconstructive options, and very short estimates could help identify those who will not survive 1 month and should not undergo surgery. Thereby, an important use of this tool would be to help avoid unsuccessful and expensive surgery during the last month of life.
Questions/purposes: We seek to provide a reliable, objective means of estimating survival in patients with metastatic bone disease. After generating models to derive 1- and 6-month survival estimates, we determined suitability for clinical use by applying receiver operator characteristic (ROC) (area under the curve [AUC] > 0.7) and decision curve analysis (DCA), which determines whether using PATHFx can improve outcomes, but also discerns in which kinds of patients PATHFx should not be used.
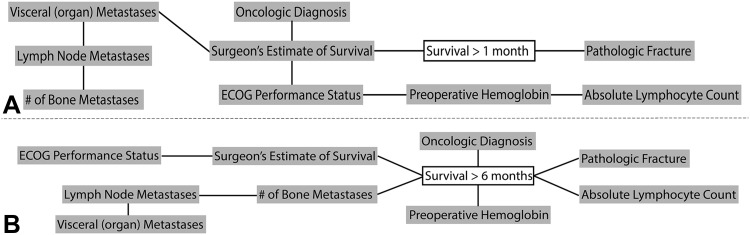
Methods: We used two, existing, skeletal metastasis registries chosen for their quality and availability. Data from Memorial Sloan-Kettering Cancer Center (training set, n = 189) was used to develop two Bayesian Belief Networks trained to estimate the likelihood of survival at 1 and 6 months after surgery. Next, data from eight major referral centers across Scandinavia (n = 815) served as the external validation set-that is, as a means to test model performance in a different patient population. The diversity of the data between the training set from Memorial Sloan-Kettering Cancer Center and the Scandinavian external validation set is important to help ensure the models are applicable to patients in various settings with differing demographics and treatment philosophies. We considered disease-specific, laboratory, and demographic information, and the surgeon's estimate of survival. For each model, we calculated the area under the ROC curve (AUC) as a metric of discriminatory ability and the Net Benefit using DCA to determine whether the models were suitable for clinical use.
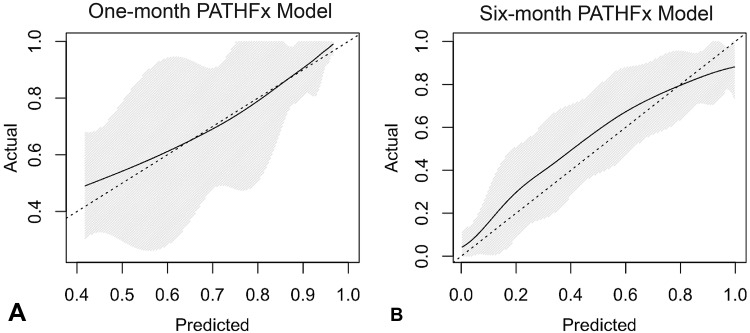
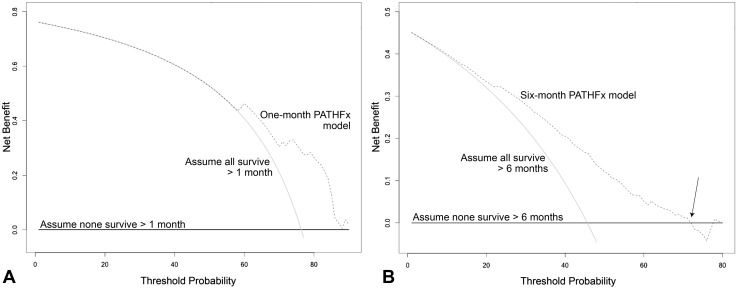
Results: On external validation, the AUC for the 1- and 6-month models were 0.76 (95% CI, 0.72-0.80) and 0.76 (95% CI, 0.73-0.79), respectively. The models conferred a positive net benefit on DCA, indicating each could be used rather than assume all patients or no patients would survive greater than 1 or 6 months, respectively.
Conclusions: Decision analysis confirms that the 1- and 6-month Bayesian models are suitable for clinical use.
Clinical relevance: These data support upgrading www.pathfx.org with the algorithms described above, which is designed to guide surgical decision-making, and function as a risk stratification method in support of clinical trials. This updating has been done, so now surgeons may use any web browser to generate survival estimates at 1, 3, 6, and 12 months after surgery, at no cost. Just as short estimates of survival help justify palliative therapy or less-invasive approaches to stabilization, more favorable survival estimates at 6 or 12 months are used to justify more durable, complicated, and expensive reconstructive options.
Figures

Comment in
-
CORR Insights®: Can We Estimate Short- and Intermediate-term Survival in Patients Undergoing Surgery for Metastatic Bone Disease?Clin Orthop Relat Res. 2017 Apr;475(4):1262-1264. doi: 10.1007/s11999-016-5200-x. Epub 2016 Dec 19. Clin Orthop Relat Res. 2017. PMID: 27995562 Free PMC article. No abstract available.
Similar articles
-
External Validation of PATHFx Version 3.0 in Patients Treated Surgically and Nonsurgically for Symptomatic Skeletal Metastases.Clin Orthop Relat Res. 2020 Apr;478(4):808-818. doi: 10.1097/CORR.0000000000001081. Clin Orthop Relat Res. 2020. PMID: 32195761 Free PMC article.
-
Can A Multivariate Model for Survival Estimation in Skeletal Metastases (PATHFx) Be Externally Validated Using Japanese Patients?Clin Orthop Relat Res. 2017 Sep;475(9):2263-2270. doi: 10.1007/s11999-017-5389-3. Epub 2017 May 30. Clin Orthop Relat Res. 2017. PMID: 28560532 Free PMC article.
-
How do we estimate survival? External validation of a tool for survival estimation in patients with metastatic bone disease-decision analysis and comparison of three international patient populations.BMC Cancer. 2015 May 22;15:424. doi: 10.1186/s12885-015-1396-5. BMC Cancer. 2015. PMID: 25998535 Free PMC article.
-
Diagnostic accuracy and receiver-operating characteristics curve analysis in surgical research and decision making.Ann Surg. 2011 Jan;253(1):27-34. doi: 10.1097/sla.0b013e318204a892. Ann Surg. 2011. PMID: 21294285 Review.
-
A Primer on Bayesian Decision Analysis With an Application to a Kidney Transplant Decision.Transplantation. 2016 Mar;100(3):489-96. doi: 10.1097/TP.0000000000001145. Transplantation. 2016. PMID: 26900809 Free PMC article. Review.
Cited by
-
Prevalence of primary malignant tumours, rates of pathological fracture, and mortality in the setting of metastatic bone disease.Bone Jt Open. 2023 Jun 5;4(6):424-431. doi: 10.1302/2633-1462.46.BJO-2023-0042.R1. Bone Jt Open. 2023. PMID: 37272304 Free PMC article.
-
CORR Insights®: Can Machine-learning Techniques Be Used for 5-year Survival Prediction of Patients With Chondrosarcoma?Clin Orthop Relat Res. 2018 Oct;476(10):2049-2051. doi: 10.1097/CORR.0000000000000474. Clin Orthop Relat Res. 2018. PMID: 30179925 Free PMC article. No abstract available.
-
Prognosis by cancer type and incidence of zoledronic acid-related osteonecrosis of the jaw: a single-center retrospective study.Support Care Cancer. 2022 May;30(5):4505-4514. doi: 10.1007/s00520-022-06839-4. Epub 2022 Feb 3. Support Care Cancer. 2022. PMID: 35113225
-
Comparison of Two Modern Survival Prediction Tools, SORG-MLA and METSSS, in Patients With Symptomatic Long-bone Metastases Who Underwent Local Treatment With Surgery Followed by Radiotherapy and With Radiotherapy Alone.Clin Orthop Relat Res. 2024 Dec 1;482(12):2193-2208. doi: 10.1097/CORR.0000000000003185. Epub 2024 Jul 23. Clin Orthop Relat Res. 2024. PMID: 39051924
-
External Validation of PATHFx Version 3.0 in Patients Treated Surgically and Nonsurgically for Symptomatic Skeletal Metastases.Clin Orthop Relat Res. 2020 Apr;478(4):808-818. doi: 10.1097/CORR.0000000000001081. Clin Orthop Relat Res. 2020. PMID: 32195761 Free PMC article.
References
-
- Forsberg JA. Suggested Guidelines. In: Wedin R, Bauer H, Weidenhielm L, editors. Turning Data Into Decisions. Stockholm: Sweden, Karolinska University Press; 2015. pp. 56–57.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
