

The value of quality of life assessment in chronic myeloid leukemia patients receiving tyrosine kinase inhibitors
- PMID: 27913477
- PMCID: PMC6142524
- DOI: 10.1182/asheducation-2016.1.170
The value of quality of life assessment in chronic myeloid leukemia patients receiving tyrosine kinase inhibitors
Abstract
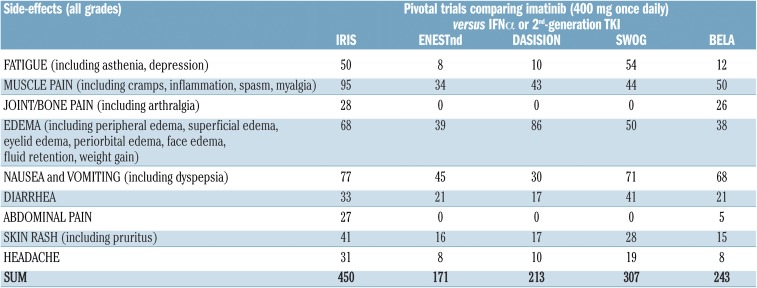
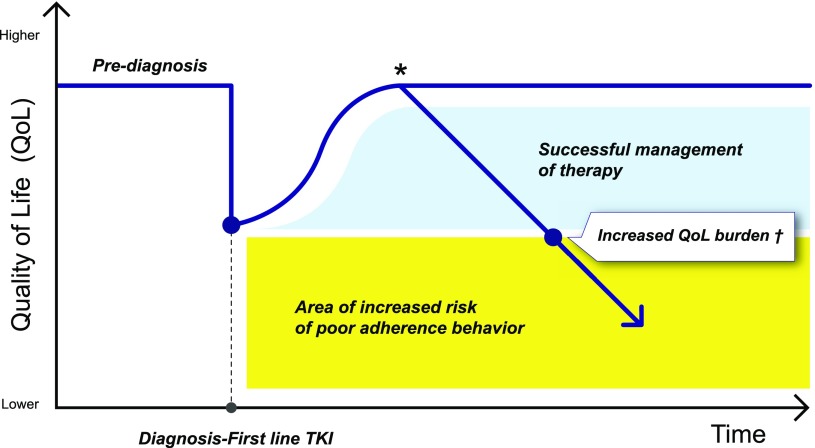
The development of the oral tyrosine kinase inhibitors (TKIs) to treat chronic myeloid leukemia (CML) is one of the great triumphs of cancer research. Although the efficacy of TKIs has dramatically improved the disease-specific overall survival rate, the prevalence of CML is increasing worldwide. Currently, CML patients receive prolonged (even lifelong) treatment, and over the last decade, clinical decision making has become challenging. Therefore, consideration of the effects of TKI therapies on patients' quality of life (QoL) and symptom burden (ie, patient-reported outcomes [PROs]) is now critical to more robustly inform patient care and improve health care quality. Over the last 5 years, a number of studies have generated valuable PRO data, for example, on long-term QoL effects of imatinib therapy or symptom burden of patients switching from imatinib to second-generation TKIs. PRO findings are important, as they provide a unique patient perspective on the burden of the disease and treatments effects. We will review main evidence-based data on the use of PROs in clinical research and highlight the importance of methodological rigor of PRO assessment. Also, we will describe the potential value of using PRO assessment in routine clinical practice, for example, to facilitate timely management of side effects. Areas for future research will also be discussed.
© 2016 by The American Society of Hematology. All rights reserved.
Conflict of interest statement
Conflict-of-interest disclosure: F.E. has received research funding from Lundbeck and TEVA and has consulted for Seattle Genetics, TEVA, and Bristol-Myers Squibb. L.C. declares no competing financial interests.
Figures
References
-
- Deininger M, O’Brien SG, Guilhot F, et al. International randomized study of interferon vs STI571 (IRIS) 8-year follow up: sustained survival and low risk for Progression or events in patients with newly diagnosed chronic myeloid leukemia in chronic phase (CML-CP) treated with imatinib [abstract]. Blood. 2009;114(22):462.
-
- Höglund M, Sandin F, Simonsson B. Epidemiology of chronic myeloid leukaemia: an update. Ann Hematol. 2015;94(suppl 2):S241-S247. - PubMed
-
- Gambacorti-Passerini C, Antolini L, Mahon FX, et al. Multicenter independent assessment of outcomes in chronic myeloid leukemia patients treated with imatinib. J Natl Cancer Inst. 2011;103(7):553-561. - PubMed
-
- Cortes JE, Saglio G, Baccarani M, et al. Final study results of the phase 3 dasatinib versus imatinib in newly diagnosed chronic myeloid leukemia in chronic phase (CML-CP) trial (DASISION, CA180-056) [abstract]. Blood. 2014;124(21):152.
-
- Hochhaus A, Saglio G, Hughes TP, et al. Impact of treatment with frontline nilotinib (NIL) vs imatinib (IM) on sustained deep molecular response (MR) in patients (pts) with newly diagnosed chronic myeloid leukemia in chronic phase (CML-CP) [abstract]. Blood. 2015;126(23):2781.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous