

Long-term risk of second malignancy and cardiovascular disease after Hodgkin lymphoma treatment
- PMID: 27913498
- PMCID: PMC6142518
- DOI: 10.1182/asheducation-2016.1.323
Long-term risk of second malignancy and cardiovascular disease after Hodgkin lymphoma treatment
Abstract
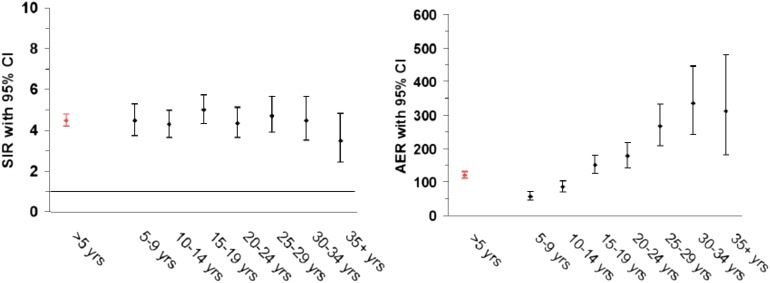
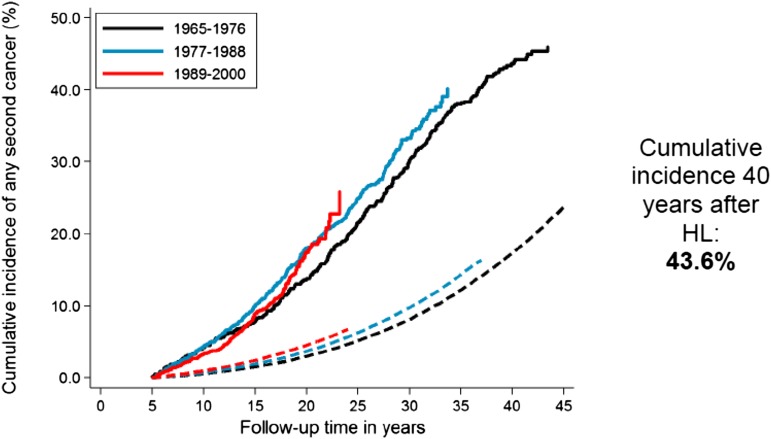
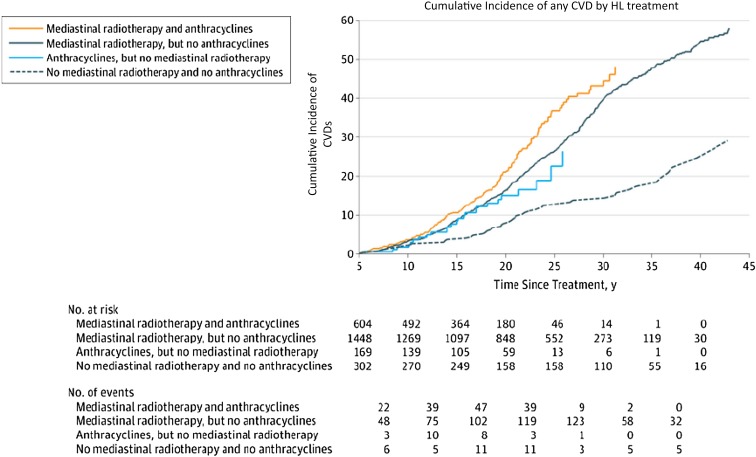
Long-term survivors of Hodgkin lymphoma (HL) experience several late adverse effects of treatment, with second malignant neoplasms (SMNs) and cardiovascular diseases (CVDs) being the leading causes of death in these patients. Other late effects have also been identified, such as pulmonary dysfunction, endocrinopathies (thyroid dysfunction, infertility), neck muscle atrophy, and persistent fatigue. HL survivors have two- to fourfold increased risks to develop SMNs and CVD compared with the general population. With respect to SMNs, radiotherapy is associated with 1.5- to 15-fold increased risk of solid malignancies. The relative risk (RR) of solid tumors increases steadily with increasing follow-up time from 5 to 15 years since radiotherapy, and remains elevated for at least 40 years. The RR of solid SMNs increases strongly with younger age at first treatment. Risks of lung, breast, and gastrointestinal (GI) cancers increase with higher radiation dose. Alkylating agent chemotherapy, especially procarbazine, does not only increase risk of leukemia but also of solid malignancies, in particular, cancers of the lung and GI tract. In contrast, gonadotoxic chemotherapy decreases the risk of radiation-associated breast cancer, through induction of premature menopause. Smoking appears to multiply the radiation- and chemotherapy-associated risks of lung cancer. Both radiotherapy and chemotherapy for HL may cause cardiovascular toxicity. Radiotherapy increases the risk of coronary heart disease, valvular heart disease, congestive heart failure (HF), and pericarditis, whereas anthracycline-containing chemotherapy increases the risks of HF and valvular heart disease. Cardiovascular toxicity following radiotherapy is usually observed from 5 to at least 35 years after therapy, whereas anthracycline-related toxicity is already observed during treatment, up to at least 25 years. The joint effects of anthracyclines, radiotherapy, and conventional cardiovascular risk factors (eg, hypertension, smoking, and physical inactivity) appear to be additive rather than multiplicative. HL survivors need lifelong risk-based screening for selected SMNs and CVDs. Furthermore, preventive strategies should include lifestyle and drug-based interventions to minimize exposure to conventional risk factors for cancer and CVD.
© 2016 by The American Society of Hematology. All rights reserved.
Conflict of interest statement
Conflict-of-interest disclosure: The authors declare no competing financial interests.
Figures
References
-
- Favier O, Heutte N, Stamatoullas-Bastard A, et al. ; European Organization for Research and Treatment of Cancer (EORTC) Lymphoma Group and the Groupe d’Etudes des Lymphomes de l’Adulte (GELA). Survival after Hodgkin lymphoma: causes of death and excess mortality in patients treated in 8 consecutive trials. Cancer. 2009;115(8):1680-1691. - PubMed
-
- Ng AK, Bernardo MP, Weller E, et al. . Long-term survival and competing causes of death in patients with early-stage Hodgkin’s disease treated at age 50 or younger. J Clin Oncol. 2002;20(8):2101-2108. - PubMed
-
- Kiserud CE, Loge JH, Fosså A, Holte H, Cvancarova M, Fosså SD. Mortality is persistently increased in Hodgkin’s lymphoma survivors. Eur J Cancer. 2010;46(9):1632-1639. - PubMed
-
- Hodgson DCGE, Grunfeld E, Gunraj N, Del Giudice L. A population-based study of follow-up care for Hodgkin lymphoma survivors: opportunities to improve surveillance for relapse and late effects. Cancer. 2010;116(14):3417-3425. - PubMed
-
- Aleman BM, van den Belt-Dusebout AW, Klokman WJ, Van’t Veer MB, Bartelink H, van Leeuwen FE. Long-term cause-specific mortality of patients treated for Hodgkin’s disease. J Clin Oncol. 2003;21(18):3431-3439. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous