

Myelodysplastic and myeloproliferative disorders of childhood
- PMID: 27913534
- PMCID: PMC6142519
- DOI: 10.1182/asheducation-2016.1.598
Myelodysplastic and myeloproliferative disorders of childhood
Abstract
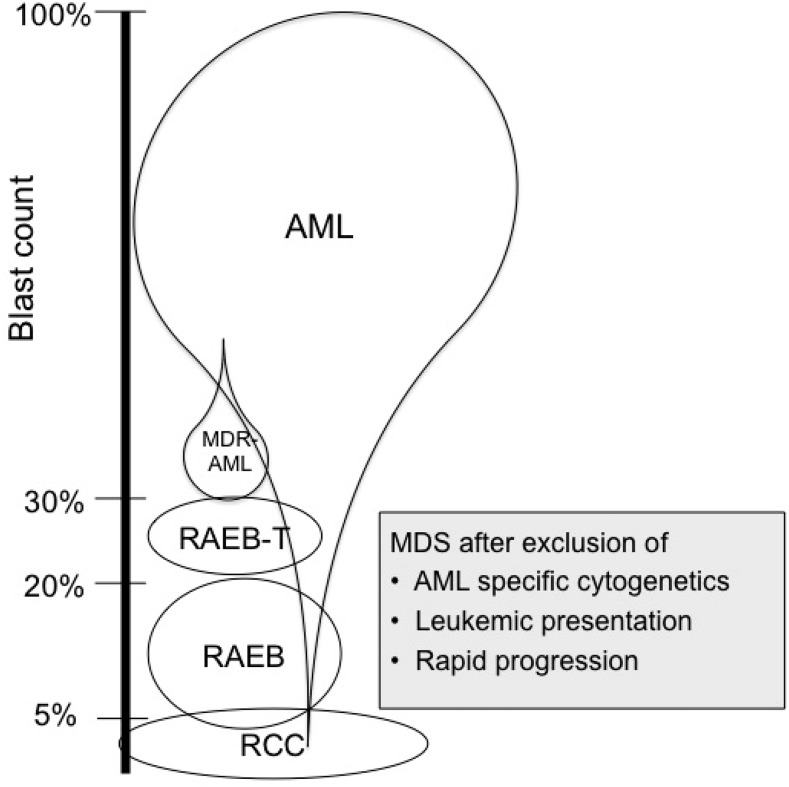
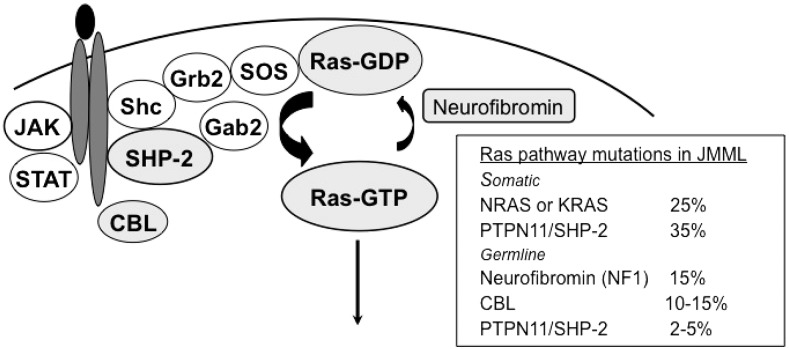
Myelodysplastic syndrome (MDS) and myeloproliferative disorders are rare in children; they are divided into low-grade MDS (refractory cytopenia of childhood [RCC]), advanced MDS (refractory anemia with excess blasts in transformation), and juvenile myelomonocytic leukemia (JMML), each with different characteristics and management strategies. Underlying genetic predisposition is recognized in an increasing number of patients. Germ line GATA2 mutation is found in 70% of adolescents with MDS and monosomy 7. It is challenging to distinguish RCC from aplastic anemia, inherited bone marrow failure, and reactive conditions. RCC is often hypoplastic and may respond to immunosuppressive therapy. In case of immunosuppressive therapy failure, hypercellular RCC, or RCC with monosomy 7, hematopoietic stem cell transplantation (HSCT) using reduced-intensity conditioning regimens is indicated. Almost all patients with refractory anemia with excess blasts are candidates for HSCT; children age 12 years or older have a higher risk of treatment-related death, and the conditioning regimens should be adjusted accordingly. Unraveling the genetics of JMML has demonstrated that JMML in patients with germ line PTPN11 and CBL mutations often regresses spontaneously, and therapy is seldom indicated. Conversely, patients with JMML and neurofibromatosis type 1, somatic PTPN11, KRAS, and most of those with NRAS mutations have a rapidly progressive disease, and early HSCT is indicated. The risk of relapse after HSCT is high, and prophylaxis for graft-versus-host disease and monitoring should be adapted to this risk.
© 2016 by The American Society of Hematology. All rights reserved.
Conflict of interest statement
Conflict-of-interest disclosures: The author declares no competing financial interests.
Figures
References
-
- Hasle H, Niemeyer CM, Chessells JM, et al. . A pediatric approach to the WHO classification of myelodysplastic and myeloproliferative diseases. Leukemia. 2003;17(2):277-282. - PubMed
-
- Swerdlow SH, Campo E, Harris NL, et al. . WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. Lyon, France: IARC; 2008
-
- Hasegawa D. The current perspective of low-grade myelodysplastic syndrome in children. Int J Hematol. 2016;103(4):360-364. - PubMed
-
- Locatelli F, Niemeyer CM. How I treat juvenile myelomonocytic leukemia. Blood. 2015;125(7):1083-1090. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous