

A Randomized Trial of Displaying Paid Price Information on Imaging Study and Procedure Ordering Rates
- PMID: 27913910
- PMCID: PMC5377881
- DOI: 10.1007/s11606-016-3917-6
A Randomized Trial of Displaying Paid Price Information on Imaging Study and Procedure Ordering Rates
Abstract
Background: Prior studies have demonstrated how price transparency lowers the test-ordering rates of trainees in hospitals, and physician-targeted price transparency efforts have been viewed as a promising cost-controlling strategy.
Objective: To examine the effect of displaying paid-price information on test-ordering rates for common imaging studies and procedures within an accountable care organization (ACO).
Design: Block randomized controlled trial for 1 year.
Subjects: A total of 1205 fully licensed clinicians (728 primary care, 477 specialists).
Intervention: Starting January 2014, clinicians in the Control arm received no price display; those in the intervention arms received Single or Paired Internal/External Median Prices in the test-ordering screen of their electronic health record. Internal prices were the amounts paid by insurers for the ACO's services; external paid prices were the amounts paid by insurers for the same services when delivered by unaffiliated providers.
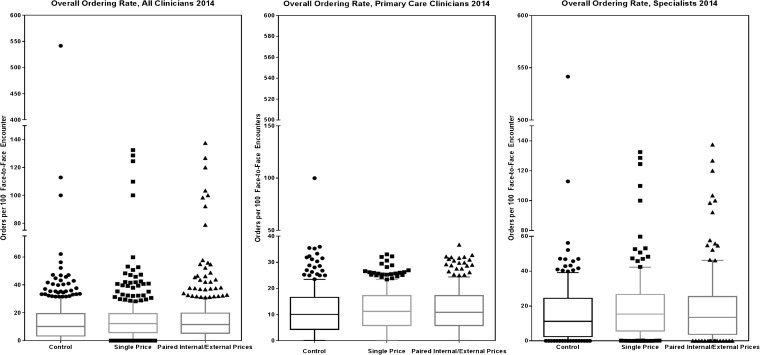
Main measures: Ordering rates (orders per 100 face-to-face encounters with adult patients): overall, designated to be completed internally within the ACO, considered "inappropriate" (e.g., MRI for simple headache), and thought to be "appropriate" (e.g., screening colonoscopy).
Key results: We found no significant difference in overall ordering rates across the Control, Single Median Price, or Paired Internal/External Median Prices study arms. For every 100 encounters, clinicians in the Control arm ordered 15.0 (SD 31.1) tests, those in the Single Median Price arm ordered 15.0 (SD 16.2) tests, and those in the Paired Prices arms ordered 15.7 (SD 20.5) tests (one-way ANOVA p-value 0.88). There was no difference in ordering rates for tests designated to be completed internally or considered to be inappropriate or appropriate.
Conclusions: Displaying paid-price information did not alter how frequently primary care and specialist clinicians ordered imaging studies and procedures within an ACO. Those with a particular interest in removing waste from the health care system may want to consider a variety of contextual factors that can affect physician-targeted price transparency.
Keywords: electronic health record; health services research; randomized trials.
Conflict of interest statement
Contributors
We appreciate the assistance our organizational partner, Atrius Health, provided for this study.
Funder
This work was financially supported by the Robert Wood Johnson Foundation Health Care Financing Organization.
Prior Presentations
This paper received a “Best Abstract” Award at the 2015 AcademyHealth Annual Research Meeting, the premier meeting for health services research. This study was also presented at the 2015 Society of General Internal Medicine Annual Meeting.
Financial Disclosure
The authors have no financial relationships relevant to this article to disclose. The sponsor had no role in the design and conduct of the study; in the collection, analysis, and interpretation of the data; or in the preparation, review, or approval of the manuscript or the decision to submit.
Conflict of Interest
The authors have no conflicts of interest to disclose, except Dr. Thomas D. Sequist is a member on Aetna’s Racial and Ethnic Equality Committee. The content of this manuscript is solely the responsibility of the authors and does not represent the official views of the Veterans Health Administration, the National Center for Ethics in Health Care, or the US Government.
Authorship
Alyna T. Chien: Dr. Chien conceptualized and designed the study; acquired, analyzed and interpreted the data; drafted the initial and critically revised the manuscript; obtained funding, provided administrative, technical, and material support; had full access to all of the data in the study; and takes responsibility for the integrity of the data and the accuracy of the data analysis. Kate E. Koplan, Lisa S. Lehmann and Anna D. Sinaiko: Drs. Koplan, Lehmann and Sinaiko interpreted the data and critically revised the manuscript. Laura A. Hatfield, Carter R. Petty: Dr. Hatfield and Mr. Petty analyzed and interpreted the data, and critically revised the manuscript. Meredith B. Rosenthal and Thomas D. Sequist: Drs. Rosenthal and Sequist conceptualized and designed the study; interpreted the data; critically revised the manuscript, and obtained funding.
Figures
Comment in
-
Capsule Commentary on Chien et al., A Randomized Trial of Displaying Paid Price Information on Imaging Study and Procedure Ordering Rates.J Gen Intern Med. 2017 Apr;32(4):472. doi: 10.1007/s11606-017-3984-3. J Gen Intern Med. 2017. PMID: 28097608 Free PMC article. No abstract available.
References
-
- Boyd C, Darer J, Boult C, Fried L. Clinical practice guidelines and quality of care for older patients with multiple comorbid diseases: implications for pay for performance. JAMA. 2005;294(6). http://jama.jamanetwork.com/article.aspx?articleid=201377. Accessed 21 Oct 2016. - PubMed
-
- Crosson F. Change the microenvironment. Delivery system reform essential to control costs. Mod Healthc. 2009;27(39):20–21. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
